Você também pode gostar
- Braddock's Classic WritingsDocumento172 páginasBraddock's Classic WritingsBraddock www.braddocksblog.com100% (6)
- Promoting Comfort, Rest and SleepDocumento59 páginasPromoting Comfort, Rest and Sleepkarendelarosa0627775% (4)
- Flanders Fields Shared Reading LessonDocumento2 páginasFlanders Fields Shared Reading Lessonapi-289261661Ainda não há avaliações
- Peran Akupunktur Medik Pada Kasus NyeriDocumento155 páginasPeran Akupunktur Medik Pada Kasus NyeriSilvia HandikaAinda não há avaliações
- Pain Hand OutsDocumento9 páginasPain Hand OutsAnonymous BBs1xxk96V100% (1)
- PainDocumento29 páginasPainjolilarmatarAinda não há avaliações
- Mod08 Pain Class1 PivotDocumento52 páginasMod08 Pain Class1 PivotRafaelAinda não há avaliações
- Pathophysiology of PainDocumento52 páginasPathophysiology of PainTahta Pambudi100% (3)
- Pathophysiology and Managemement of Pain: Dr. Subodh Kumar Mahto, Dept. of Medicine Pgimer, DR - RML Hospital. NEW DelhiDocumento86 páginasPathophysiology and Managemement of Pain: Dr. Subodh Kumar Mahto, Dept. of Medicine Pgimer, DR - RML Hospital. NEW DelhiMarcelo GutiérrezAinda não há avaliações
- Patofisiologi NyeriDocumento99 páginasPatofisiologi NyeriWandi WDAinda não há avaliações
- Pain and Pain ManagementDocumento22 páginasPain and Pain ManagementChen Li100% (1)
- PainDocumento23 páginasPainAbo De7kaAinda não há avaliações
- Assessin G: Karelle Custodia Theresa GalivoDocumento23 páginasAssessin G: Karelle Custodia Theresa GalivoKarelle CustodiaAinda não há avaliações
- Pain ManagementDocumento11 páginasPain ManagementLokeshwari KatreAinda não há avaliações
- Pain Physiology PathologyDocumento71 páginasPain Physiology Pathologykeerthi_keshapagaAinda não há avaliações
- P A I N 1my Power PointDocumento38 páginasP A I N 1my Power Pointapi-3697326100% (1)
- Physiology of Pain Pathways and Its Modulation: DR HassanDocumento79 páginasPhysiology of Pain Pathways and Its Modulation: DR HassanvaishnaviAinda não há avaliações
- Prof. H.Gusbakti, MSC, PKK, AifmDocumento74 páginasProf. H.Gusbakti, MSC, PKK, AifmBudy RahmantoAinda não há avaliações
- Lecture - 12 2013Documento28 páginasLecture - 12 2013LucjaAinda não há avaliações
- Management of Acute Pain: ANLS 2012 Jakarta, 5-6 Januari 2013Documento44 páginasManagement of Acute Pain: ANLS 2012 Jakarta, 5-6 Januari 2013harry hadi saputraAinda não há avaliações
- Management of Acute Pain: ANLS 2012Documento41 páginasManagement of Acute Pain: ANLS 2012aldodongAinda não há avaliações
- Margo Mccaffery, A Nurse and A Pioneer in Pain ManagementDocumento7 páginasMargo Mccaffery, A Nurse and A Pioneer in Pain ManagementGiselle Chloe Baluya ico100% (1)
- About This Article: Basics of Pain ControlDocumento22 páginasAbout This Article: Basics of Pain ControlJailan IbrahimAinda não há avaliações
- Physiology of PainDocumento43 páginasPhysiology of PainNashwan AAinda não há avaliações
- 1 Pain Sensation Physiology DR Ambreen TauseefDocumento73 páginas1 Pain Sensation Physiology DR Ambreen TauseefbilalAinda não há avaliações
- An Introduction To Pain Pathways 2022Documento9 páginasAn Introduction To Pain Pathways 2022widad syairoziAinda não há avaliações
- 4th Lec. Pain and Orofacial PainDocumento145 páginas4th Lec. Pain and Orofacial Painعبدالوهاب صلاحAinda não há avaliações
- Midterm MS3 (1 & 2)Documento4 páginasMidterm MS3 (1 & 2)Rheeanne Mae AmilasanAinda não há avaliações
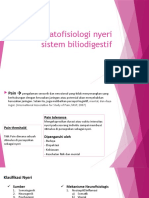
- Patofisiologi Nyeri Sistem BiliodigestifDocumento22 páginasPatofisiologi Nyeri Sistem BiliodigestifNathaniaAinda não há avaliações
- Nyeri Nosiseptif Sup - XIDocumento82 páginasNyeri Nosiseptif Sup - XIDiana SariAinda não há avaliações
- Dr. Nurhayu Ab RahmanDocumento24 páginasDr. Nurhayu Ab RahmanHotaru ImaiAinda não há avaliações
- Pengelolaan Nyeri: Joko MurdiyantoDocumento55 páginasPengelolaan Nyeri: Joko Murdiyantodwi agus yuliantoAinda não há avaliações
- Physiology of PainDocumento30 páginasPhysiology of PainVaibhavJain100% (1)
- Neurobiology of Pain: C R MishraDocumento47 páginasNeurobiology of Pain: C R MishraKing Bradley100% (2)
- Module 2M: Concept of PainDocumento3 páginasModule 2M: Concept of PainDominic DegraciaAinda não há avaliações
- Pain PathwaysDocumento45 páginasPain PathwaysKabirAinda não há avaliações
- Management of Acute PainDocumento76 páginasManagement of Acute PainAnonymous nruHyuwtJ100% (1)
- Chronic Pain Management: Dr. Ankit GajjarDocumento74 páginasChronic Pain Management: Dr. Ankit GajjarDivya Rekha KolliAinda não há avaliações
- The Anatomy Physiology PainDocumento5 páginasThe Anatomy Physiology PaincrownesyaAinda não há avaliações
- Management Acute PainDocumento110 páginasManagement Acute PainjohannesAinda não há avaliações
- MECHANISM OF PAIN (University Question)Documento14 páginasMECHANISM OF PAIN (University Question)AkhilaAinda não há avaliações
- Day 1 - Doc Session 1 - Patho Physiology of Pain - DR BijiDocumento69 páginasDay 1 - Doc Session 1 - Patho Physiology of Pain - DR Bijim debAinda não há avaliações
- Unit 1 OT Methods NotesDocumento5 páginasUnit 1 OT Methods NotesJenny RajanAinda não há avaliações
- Materi Kuliah Pain Patophysiology Ima 2017Documento62 páginasMateri Kuliah Pain Patophysiology Ima 2017Putu DesyAinda não há avaliações
- Intr Oduction: Classification of PainDocumento4 páginasIntr Oduction: Classification of Painanimesh panda100% (1)
- Ncm112 LecDocumento7 páginasNcm112 LecKylle AlimosaAinda não há avaliações
- The Neurophysiology of PainDocumento11 páginasThe Neurophysiology of Painliveconnectionz282Ainda não há avaliações
- Assessment: PainDocumento7 páginasAssessment: PainNathan BarrerasAinda não há avaliações
- DR Yuneldi Anwar Sps (K) Bagian Neurologi Fk-Usu/ Rsup H. Adam Malik MedanDocumento59 páginasDR Yuneldi Anwar Sps (K) Bagian Neurologi Fk-Usu/ Rsup H. Adam Malik MedanZikri Putra Lan LubisAinda não há avaliações
- Mechanisms, Classification and Assesment: Departemen Neurologi Fakutas Kedokteran Universitas Islam Sumatera UtaraDocumento49 páginasMechanisms, Classification and Assesment: Departemen Neurologi Fakutas Kedokteran Universitas Islam Sumatera UtaraDea indah damayantiAinda não há avaliações
- Kuliah Mekanisme Sensorik & Keseimbangan - DR SonnyDocumento47 páginasKuliah Mekanisme Sensorik & Keseimbangan - DR SonnyYuke PutriAinda não há avaliações
- AnalgesicsDocumento11 páginasAnalgesicsNafisa TasnimAinda não há avaliações
- Assessment of PainDocumento6 páginasAssessment of PainFitri HandayaniAinda não há avaliações
- Pain PDFDocumento46 páginasPain PDFwokorowAinda não há avaliações
- Pain Control TheoryDocumento24 páginasPain Control TheorySwathy AshokAinda não há avaliações
- Pain SeminarDocumento25 páginasPain SeminarsruthiAinda não há avaliações
- Pain Basic Consideration PDFDocumento4 páginasPain Basic Consideration PDFCiprian CorneaAinda não há avaliações
- PAINDocumento46 páginasPAINShivam SoniAinda não há avaliações
- 3 DR Hery - Pain Management 2018Documento58 páginas3 DR Hery - Pain Management 2018SATIYO SATIYOAinda não há avaliações
- OmrDocumento39 páginasOmrabhijeetAinda não há avaliações
- 3 +Pain+2018+PDF+1ppDocumento33 páginas3 +Pain+2018+PDF+1pphorace_linAinda não há avaliações
- Background: Hogan D J, Mason S H. 2011. Lichen Simplex Chronicus. Diakses DariDocumento1 páginaBackground: Hogan D J, Mason S H. 2011. Lichen Simplex Chronicus. Diakses DariPatresya LantanAinda não há avaliações
- Jurnal ReadingDocumento27 páginasJurnal ReadingPatresya LantanAinda não há avaliações
- Jurnal ReadingDocumento27 páginasJurnal ReadingPatresya LantanAinda não há avaliações
- Musculoskeletal RadiologyDocumento103 páginasMusculoskeletal RadiologyPatresya LantanAinda não há avaliações
- Polymorphic Eruption of PregnancyDocumento8 páginasPolymorphic Eruption of PregnancyPatresya LantanAinda não há avaliações
- Journal Reading CardiologyDocumento33 páginasJournal Reading CardiologyPatresya LantanAinda não há avaliações
- Jurnal Mata Besifloxacin Opthalmic SuspensionDocumento13 páginasJurnal Mata Besifloxacin Opthalmic SuspensionPatresya LantanAinda não há avaliações
- Asma TerkontrolDocumento4 páginasAsma TerkontrolPatresya LantanAinda não há avaliações
- Length/height-For-Age BOYS: Birth To 5 Years (Z-Scores)Documento1 páginaLength/height-For-Age BOYS: Birth To 5 Years (Z-Scores)Malisa LukmanAinda não há avaliações
- Skin in PreggnancyDocumento120 páginasSkin in PreggnancyPatresya LantanAinda não há avaliações
- Penny R. Thayer, FNP, BC Gastro/Hepatology NP James H. Quillen, VAMCDocumento27 páginasPenny R. Thayer, FNP, BC Gastro/Hepatology NP James H. Quillen, VAMCPatresya LantanAinda não há avaliações
- Pengantar (Fix)Documento21 páginasPengantar (Fix)ubayyumrAinda não há avaliações
- JurnalDocumento24 páginasJurnalPatresya LantanAinda não há avaliações
- ZIDOVUDINE-RCOG Guideline On HIV in PregnancyDocumento12 páginasZIDOVUDINE-RCOG Guideline On HIV in PregnancyFarah AzizahAinda não há avaliações
- Typhoid JournalDocumento10 páginasTyphoid JournalPatresya LantanAinda não há avaliações
- Pain+Management1+4 4 13Documento53 páginasPain+Management1+4 4 13Anonymous 75TDy2yAinda não há avaliações
- Dengue Who ProtocolDocumento48 páginasDengue Who ProtocolPatresya LantanAinda não há avaliações
- Lepto Spiros IsDocumento22 páginasLepto Spiros IsAhmad AbdulahabAinda não há avaliações
- Otitis MediaDocumento44 páginasOtitis MediaPatresya LantanAinda não há avaliações
- Penyakit CacingDocumento17 páginasPenyakit CacingayuAinda não há avaliações
- ThrombosisDocumento38 páginasThrombosisDiana PanaitAinda não há avaliações
- Malaria BeratDocumento19 páginasMalaria BeratadhyraafAinda não há avaliações
- HT Pregnancy Guideline July 2014Documento52 páginasHT Pregnancy Guideline July 2014Mary OrtegaAinda não há avaliações
- Lepto Spiros IsDocumento22 páginasLepto Spiros IsAhmad AbdulahabAinda não há avaliações
- Vitamins and MineralsDocumento25 páginasVitamins and MineralsFyan FiradyAinda não há avaliações
- Dystocia SOGCDocumento16 páginasDystocia SOGCAdhitia NugrahantoAinda não há avaliações
- Stent-Retriever Thrombectomy After Intravenous T-PA vs. T-PA Alone in StrokeDocumento20 páginasStent-Retriever Thrombectomy After Intravenous T-PA vs. T-PA Alone in StrokePatresya LantanAinda não há avaliações
- Pain+Management1+4 4 13Documento53 páginasPain+Management1+4 4 13Anonymous 75TDy2yAinda não há avaliações
- Jurnal Mata Besifloxacin Opthalmic SuspensionDocumento13 páginasJurnal Mata Besifloxacin Opthalmic SuspensionPatresya LantanAinda não há avaliações
- Tarot Spread For Finding Lost Items - Find Lost Things Fast!Documento7 páginasTarot Spread For Finding Lost Items - Find Lost Things Fast!vojkan73Ainda não há avaliações
- GFPP3113 Politik Ekonomi AntarabangsaDocumento11 páginasGFPP3113 Politik Ekonomi AntarabangsaBangYongGukAinda não há avaliações
- Specific Learning DisabilitiesDocumento22 páginasSpecific Learning Disabilitiesapi-313062611Ainda não há avaliações
- Sas1 Gen 002Documento21 páginasSas1 Gen 002Luna ValeriaAinda não há avaliações
- Chakras EnneagramDocumento3 páginasChakras Enneagramfernandeantonio7961100% (4)
- Entrepreneurship and EnvironmentDocumento19 páginasEntrepreneurship and EnvironmentMURALI100% (1)
- Iseki Full Set Parts Catalogue DVDDocumento22 páginasIseki Full Set Parts Catalogue DVDjayflores240996web100% (134)
- Teori J.B HeatonDocumento4 páginasTeori J.B HeatonNeny M. DjamarisAinda não há avaliações
- (MCP1617) Qustionnaire-GPoA Concepcion, JerichoDocumento20 páginas(MCP1617) Qustionnaire-GPoA Concepcion, JerichoCep PyAinda não há avaliações
- Pedagogical Representation of Visual Images in EFL Textbooks - A Multimodal Perspective PDFDocumento17 páginasPedagogical Representation of Visual Images in EFL Textbooks - A Multimodal Perspective PDFEga -Dwi Arie Megawati-Ainda não há avaliações
- Art AppreciationDocumento4 páginasArt AppreciationJhan Carlo M BananAinda não há avaliações
- PIBC LogBook Guide&Samples Jun2012Documento12 páginasPIBC LogBook Guide&Samples Jun2012GOKUL PRASADAinda não há avaliações
- Building A Christ Centered Marr - John StangeDocumento31 páginasBuilding A Christ Centered Marr - John StangehungrynicetiesAinda não há avaliações
- How To Give Constructive Feedback in 6 Easy StepsDocumento3 páginasHow To Give Constructive Feedback in 6 Easy StepsolmezestAinda não há avaliações
- 12 Characteristics of An Effective TeacherDocumento4 páginas12 Characteristics of An Effective TeacherRamonitoElumbaringAinda não há avaliações
- Monthly Paid Scales 2022 2025Documento32 páginasMonthly Paid Scales 2022 2025horace smallingAinda não há avaliações
- Emotional Intelligence Theory (EQ - Emotional Quotient)Documento3 páginasEmotional Intelligence Theory (EQ - Emotional Quotient)eamAinda não há avaliações
- Neurophone CompleteDocumento9 páginasNeurophone CompleteSimon Benjamin100% (3)
- Tinnitus Causes and TreatmentDocumento3 páginasTinnitus Causes and TreatmentTinnituscausesandtreatment Tinnituscausesandtreatment100% (1)
- What Life Taught Me-Part 3Documento1 páginaWhat Life Taught Me-Part 3Karanam.RamakumarAinda não há avaliações
- 5e's ActivitiesDocumento2 páginas5e's ActivitiesJoyae ChavezAinda não há avaliações
- Expressing OpinionsDocumento8 páginasExpressing OpinionsYulia Rizki Damanik0% (1)
- The Relational Attitude in Gestalt Therapy Theory and PracticeDocumento15 páginasThe Relational Attitude in Gestalt Therapy Theory and PracticeAvtandilGogeshvili100% (1)
- HRP Final PPT Seimens Case StudyDocumento17 páginasHRP Final PPT Seimens Case StudyAmrita MishraAinda não há avaliações
- Nursing Theories and Their WorksDocumento4 páginasNursing Theories and Their WorksCharm Abyss la Morena0% (1)
- An Analysis On The Level of Satisfaction Brought by The School CanteenDocumento81 páginasAn Analysis On The Level of Satisfaction Brought by The School Canteenkyla manapat100% (5)
- Emalee CawteDocumento2 páginasEmalee Cawteapi-401329529Ainda não há avaliações
- Constructing A Replacement For The Soul - BourbonDocumento258 páginasConstructing A Replacement For The Soul - BourbonInteresting ResearchAinda não há avaliações