Você também pode gostar
- 237 Goljan Rapid Review Images FlashcardsDocumento34 páginas237 Goljan Rapid Review Images FlashcardsAhsan Tanvir100% (1)
- Ecg 01Documento103 páginasEcg 01Bandar al ghamdi100% (1)
- ACLS DrugDocumento7 páginasACLS DrugPhongsatorn Thunin100% (1)
- Hypertensive Crisis: - Alexter John C. Fajardo M.DDocumento49 páginasHypertensive Crisis: - Alexter John C. Fajardo M.DAlexter John Cabalonga FajardoAinda não há avaliações
- ADHD PresentationDocumento21 páginasADHD PresentationZainab Ali HassanAinda não há avaliações
- DKA Study GroupDocumento24 páginasDKA Study GroupAqila MumtazAinda não há avaliações
- Ventricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmDocumento2 páginasVentricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmsafasayedAinda não há avaliações
- Diagnostic Test Purpose Normal Result Nursing ResponsibilityDocumento4 páginasDiagnostic Test Purpose Normal Result Nursing Responsibilitykennethfe agron100% (1)
- ECGDocumento198 páginasECGKatrina Maravilla100% (1)
- Intra Aortic Balloon Pump (IABP) 2009Documento57 páginasIntra Aortic Balloon Pump (IABP) 2009nurminsyahAinda não há avaliações
- Nursing Care CKDDocumento17 páginasNursing Care CKDUlLfa Chii MuetmuethzAinda não há avaliações
- Wa0000.Documento7 páginasWa0000.benitez1228Ainda não há avaliações
- Norepinephrine Drug StudyDocumento2 páginasNorepinephrine Drug StudyIrish LigayaAinda não há avaliações
- OIIQ Prep QuestionsDocumento10 páginasOIIQ Prep QuestionsDan Thanh Luu67% (3)
- Permanent PacemakerDocumento23 páginasPermanent PacemakeradinsAinda não há avaliações
- Hepatic Encephalopathy: Prof. Huiling Yang Dept. PathophysiologyDocumento46 páginasHepatic Encephalopathy: Prof. Huiling Yang Dept. PathophysiologyAshish PandeyAinda não há avaliações
- Askep Kritis Sistem EndokrinDocumento37 páginasAskep Kritis Sistem EndokrinDerfina Bahagia iduAinda não há avaliações
- Kegawatan Jantung - MeDocumento41 páginasKegawatan Jantung - MeNam Min BinAinda não há avaliações
- TBR AclsDocumento9 páginasTBR Aclsric_vir_014Ainda não há avaliações
- Chronic Kidney Disease-Mineral Bone DisorderDocumento49 páginasChronic Kidney Disease-Mineral Bone DisorderÀi ZìjǐAinda não há avaliações
- Steps To Perform A Blood TransfusionDocumento1 páginaSteps To Perform A Blood Transfusionzepoli_zepoly6232Ainda não há avaliações
- Premature Ventricular ContractionDocumento17 páginasPremature Ventricular Contractiondr_jofrilAinda não há avaliações
- RevisionDocumento17 páginasRevisionMatt RenaudAinda não há avaliações
- Nursing Management: Nursing Management: Acute Kidney Injury and Chronic Kidney DiseaseDocumento22 páginasNursing Management: Nursing Management: Acute Kidney Injury and Chronic Kidney Diseasedian rachmat saputroAinda não há avaliações
- Sick Sinus Syndrome 1Documento23 páginasSick Sinus Syndrome 1Salman HabeebAinda não há avaliações
- NCP PPHDocumento2 páginasNCP PPHMark Joseph Christian100% (1)
- Reteplase (MIRel)Documento23 páginasReteplase (MIRel)Jhoann JamanilaAinda não há avaliações
- Adult Post-Cardiac Arrest Care Algorithm: o Co Io o CoDocumento1 páginaAdult Post-Cardiac Arrest Care Algorithm: o Co Io o CoKavya ShreeAinda não há avaliações
- Measurement of Cardiac Output: University College of Medical Sciences & GTB Hospital, DelhiDocumento33 páginasMeasurement of Cardiac Output: University College of Medical Sciences & GTB Hospital, DelhioctbudaAinda não há avaliações
- Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermDocumento3 páginasAssessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Objective: Short Term: Independent: Short TermMicaela CrisostomoAinda não há avaliações
- Pericardial EffusionDocumento36 páginasPericardial EffusionRizky Amalia Wakano100% (1)
- Chapter 67: Nursing Management: Shock, Systemic Inflammatory Response Syndrome, and Multiple Organ Dysfunction SyndromeDocumento8 páginasChapter 67: Nursing Management: Shock, Systemic Inflammatory Response Syndrome, and Multiple Organ Dysfunction SyndromejefrocAinda não há avaliações
- PPH Introduction 1Documento95 páginasPPH Introduction 1regine maeAinda não há avaliações
- Drug Indication Action Side Effects and Adverse Reaction Nursing ConsiderationDocumento8 páginasDrug Indication Action Side Effects and Adverse Reaction Nursing Considerationkier khierAinda não há avaliações
- Drug Study FinalDocumento6 páginasDrug Study FinalJade HemmingsAinda não há avaliações
- Nursing Care During Prenatal PeriodDocumento7 páginasNursing Care During Prenatal Periodsands32Ainda não há avaliações
- Drug StudyDocumento2 páginasDrug StudySORENI SORENIAinda não há avaliações
- Amitriptyline PDFDocumento3 páginasAmitriptyline PDFscribdseewalAinda não há avaliações
- Fluorosis: Fluoride Toxicity: Patient Management & MonitoringDocumento24 páginasFluorosis: Fluoride Toxicity: Patient Management & MonitoringdrjriAinda não há avaliações
- CABGDocumento3 páginasCABGblessed23Ainda não há avaliações
- EdemaDocumento27 páginasEdemarapadilAinda não há avaliações
- Case Study, Chapter 70, Management of Patients WithOncologic or Degenerative Neurologic DisordersDocumento1 páginaCase Study, Chapter 70, Management of Patients WithOncologic or Degenerative Neurologic Disordersclyde i am100% (1)
- Acid Base Disorders - Lecture 45Documento14 páginasAcid Base Disorders - Lecture 45yassin mostafaAinda não há avaliações
- Anaesthetic Challenges and Management of Myelomeningocele RepairDocumento6 páginasAnaesthetic Challenges and Management of Myelomeningocele RepairprastiaAinda não há avaliações
- Post Term PregnancyDocumento12 páginasPost Term PregnancyRizky Putra Ismeldi100% (1)
- Case CHFDocumento10 páginasCase CHFAgnes Erlita Distriani Patade50% (2)
- Medication: Expected Pharmacological Action Therapeutic UseDocumento1 páginaMedication: Expected Pharmacological Action Therapeutic UseclarimerAinda não há avaliações
- Case Study Bacterial MeningitisDocumento5 páginasCase Study Bacterial MeningitisChristine SaliganAinda não há avaliações
- Nursing Assessment:: Intervention Rationale Independent InterventionsDocumento2 páginasNursing Assessment:: Intervention Rationale Independent Interventionsnananana123Ainda não há avaliações
- Algorithm For Management of Acute Pulmonary Oedema PDFDocumento1 páginaAlgorithm For Management of Acute Pulmonary Oedema PDFDewi Rabiatul AkhzamiAinda não há avaliações
- Heart FailureDocumento4 páginasHeart FailureDane WrightAinda não há avaliações
- Peadiatric Advanced Life Support (Pals)Documento18 páginasPeadiatric Advanced Life Support (Pals)SREEDEVI T SURESHAinda não há avaliações
- Esophagus, TearDocumento36 páginasEsophagus, Tearapi-19641337Ainda não há avaliações
- AdrenalineDocumento2 páginasAdrenalinerazvan032006100% (1)
- Streptokinase GroupDocumento16 páginasStreptokinase GroupSuffocated LiveAinda não há avaliações
- EcgDocumento1 páginaEcgJun ManAinda não há avaliações
- Calcium GluconateDocumento1 páginaCalcium GluconateDilip SenthAinda não há avaliações
- A Drug Study On: EpinephrineDocumento16 páginasA Drug Study On: EpinephrineJay Jay JayyiAinda não há avaliações
- Oxygen Terapi Dan PrinsipelDocumento16 páginasOxygen Terapi Dan PrinsipelAmrita KaurAinda não há avaliações
- DSSSB Exam 1382017 Staff Nurse QP Prncfet - Blogspot.in PDFDocumento24 páginasDSSSB Exam 1382017 Staff Nurse QP Prncfet - Blogspot.in PDFRohan SahuAinda não há avaliações
- Product Information Avil Product NamesDocumento4 páginasProduct Information Avil Product Namesindyanexpress100% (1)
- Sub Arachnoid HaemorrageDocumento46 páginasSub Arachnoid HaemorrageShitaljit IromAinda não há avaliações
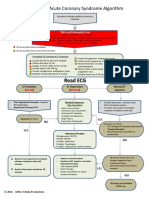
- ACLS ACS Algorithm NewDocumento3 páginasACLS ACS Algorithm Newsambo100% (1)
- ACS Algorithm 2016 PDFDocumento1 páginaACS Algorithm 2016 PDFrabin1994Ainda não há avaliações
- 12-Adult Post Resuscitation Care Algorithm 2021Documento1 página12-Adult Post Resuscitation Care Algorithm 2021khaledAinda não há avaliações
- Airway Adjuncts, Oxygenation, and VentilationDocumento32 páginasAirway Adjuncts, Oxygenation, and VentilationPuskesmas Pinang JayaAinda não há avaliações
- Airway Adjuncts, Oxygenation, and Ventilation - Paling BaruDocumento33 páginasAirway Adjuncts, Oxygenation, and Ventilation - Paling BaruPuskesmas Pinang JayaAinda não há avaliações
- Airway ManagementDocumento31 páginasAirway ManagementPuskesmas Pinang JayaAinda não há avaliações
- VF-VT AlgorithmDocumento10 páginasVF-VT AlgorithmPuskesmas Pinang JayaAinda não há avaliações
- TachycardiaDocumento12 páginasTachycardiaPuskesmas Pinang JayaAinda não há avaliações
- Diabetes Melitus Dan Tuberkulosis ParuDocumento8 páginasDiabetes Melitus Dan Tuberkulosis ParuNyoman YudiartonoAinda não há avaliações
- I. Ecologic Model A. HypothesisDocumento5 páginasI. Ecologic Model A. HypothesisTintin LevidaAinda não há avaliações
- JournalDocumento6 páginasJournalIka RachmadantAinda não há avaliações
- Case Report: Perioperative Management of A Patient With Secreting Paraganglioma Undergoing Cesarean SectionDocumento3 páginasCase Report: Perioperative Management of A Patient With Secreting Paraganglioma Undergoing Cesarean SectionYolanda FitrianiAinda não há avaliações
- 4 - Clinical Patterns in Crohn's Disease - A Statistical Study of 615 CasesDocumento9 páginas4 - Clinical Patterns in Crohn's Disease - A Statistical Study of 615 CasesVân NguyễnAinda não há avaliações
- Postpartum Haemorrhage Dr. G. Al-ShaikhDocumento51 páginasPostpartum Haemorrhage Dr. G. Al-ShaikhRaphzid InurfaceAinda não há avaliações
- Emergency Nursing IntroDocumento111 páginasEmergency Nursing IntroteuuuuAinda não há avaliações
- Knowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonDocumento17 páginasKnowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonEditor IJTSRDAinda não há avaliações
- Impacts of Antibiotic ResistanceDocumento3 páginasImpacts of Antibiotic ResistanceSajid RahimAinda não há avaliações
- EAU Pocket On Paediatric Urology 2023Documento54 páginasEAU Pocket On Paediatric Urology 2023Andrea SzaszAinda não há avaliações
- MH Guideline For Web v2Documento1 páginaMH Guideline For Web v2FilbertaAinda não há avaliações
- Liver BiopsyDocumento4 páginasLiver BiopsyLouis FortunatoAinda não há avaliações
- EFA Question BankDocumento50 páginasEFA Question BankZeeshan SyedAinda não há avaliações
- Severe Ulcerative Colitis UHL Childrens Medical GuidelineDocumento8 páginasSevere Ulcerative Colitis UHL Childrens Medical GuidelineFanny PritaningrumAinda não há avaliações
- Toxoplasmosis in PregnancyDocumento45 páginasToxoplasmosis in PregnancyTahta PambudiAinda não há avaliações
- Medial Medullary Syndrome - WikipediaDocumento8 páginasMedial Medullary Syndrome - WikipediaArun KumarAinda não há avaliações
- Level 3 Body Sleep - Sample ReportDocumento6 páginasLevel 3 Body Sleep - Sample Reportjunior browAinda não há avaliações
- Cumulative Trauma DisordersDocumento5 páginasCumulative Trauma Disordersravinaj21100% (1)
- s12944 022 01717 8Documento15 páginass12944 022 01717 8IZAMAR NADDINE LLAURE FLORESAinda não há avaliações
- Middle Ear Risk Index (MERI)Documento2 páginasMiddle Ear Risk Index (MERI)Anish RajAinda não há avaliações
- Hernia HiatalDocumento4 páginasHernia HiatalFabrizioSanchezZegarraAinda não há avaliações
- Aedes Aegypti Dengan Teknik Imunositokimia MenggunakanDocumento10 páginasAedes Aegypti Dengan Teknik Imunositokimia MenggunakanNiken CahyaningrumAinda não há avaliações
- Ecgds 09 00916Documento4 páginasEcgds 09 00916Houda El MoufidAinda não há avaliações
- Thesis Statement Examples For Eating DisordersDocumento6 páginasThesis Statement Examples For Eating Disordersjenniferontiveroskansascity100% (2)
- Parkinson's Disease Psychosis: Presentation, Diagnosis and ManagementDocumento12 páginasParkinson's Disease Psychosis: Presentation, Diagnosis and ManagementEduardo Santana SuárezAinda não há avaliações
- Introduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Documento2 páginasIntroduction & Epidemiology Clinical Features: End-Stage Renal Disease (ESRD)Nikki VillanuevaAinda não há avaliações