Você também pode gostar
- Pharmacological Classification of Drugs First EditionDocumento0 páginaPharmacological Classification of Drugs First EditionAmina BećiragićAinda não há avaliações
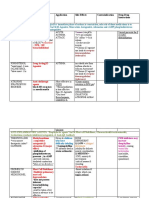
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocumento3 páginasDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinAinda não há avaliações
- Anticholinergic Drugs.Documento39 páginasAnticholinergic Drugs.Dr.Biswajit jenaAinda não há avaliações
- Cardiac GlycosidesDocumento22 páginasCardiac Glycosidesbreilano100% (1)
- Criterion-Referenced vs. Norm-Referenced AssessmentDocumento2 páginasCriterion-Referenced vs. Norm-Referenced AssessmentJohn Benedict Vocales100% (1)
- Lange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesDocumento2 páginasLange Smart Charts: Pharmacology, 2e Pharmacologic SuffixesSolAinda não há avaliações
- Antiarrhythmic Drugs Classification (Vaughan Williams)Documento8 páginasAntiarrhythmic Drugs Classification (Vaughan Williams)ana100% (1)
- Injection Blow Moulded Products Book PDFDocumento13 páginasInjection Blow Moulded Products Book PDFShafeeq AhmedAinda não há avaliações
- Peptic Ulcer Drugs and Pharmcotherapy - DrdhritiDocumento60 páginasPeptic Ulcer Drugs and Pharmcotherapy - Drdhritidbrahma100% (2)
- MOON-Score and Parts PDFDocumento9 páginasMOON-Score and Parts PDFJohn Benedict VocalesAinda não há avaliações
- Basic Trumpet PlayingDocumento14 páginasBasic Trumpet PlayingJosé Gentil Leite67% (3)
- NSAIDDocumento1 páginaNSAIDShubhangiAinda não há avaliações
- Anti-Gout DrugsDocumento38 páginasAnti-Gout Drugsapi-306036754Ainda não há avaliações
- Lecture 28 - 3rd Asessment - Sedatives, HypnoticsDocumento32 páginasLecture 28 - 3rd Asessment - Sedatives, Hypnoticsapi-3703352100% (1)
- Lecture 4, 5 - Drugs Used in Bronchial Asthma & COPDDocumento57 páginasLecture 4, 5 - Drugs Used in Bronchial Asthma & COPDBalakrishnan Thangaraj100% (1)
- Flowserve Reg PumpDocumento66 páginasFlowserve Reg Pumpshaad_ksi100% (1)
- Antihypertensive Drugs by Carewell PharmaDocumento9 páginasAntihypertensive Drugs by Carewell PharmaShyam karan YadavAinda não há avaliações
- Adverse Drug Reactions (ADRS)Documento24 páginasAdverse Drug Reactions (ADRS)ANAM IQBALAinda não há avaliações
- Summary of Adrenergic DrugsDocumento3 páginasSummary of Adrenergic DrugsrabduljabarrAinda não há avaliações
- Adrenoceptor - Activating Other Sympathomimetic Drugs PDFDocumento43 páginasAdrenoceptor - Activating Other Sympathomimetic Drugs PDFRupal RaghuwanshiAinda não há avaliações
- Alpha BlockersDocumento17 páginasAlpha BlockersKashis SharmaAinda não há avaliações
- Sedative HypnoticsDocumento27 páginasSedative HypnoticsPrecious FulgarinasAinda não há avaliações
- Sulfonamides: By: Dr. Shruthi Rammohan Final Year PG Pharmacology RRMCHDocumento45 páginasSulfonamides: By: Dr. Shruthi Rammohan Final Year PG Pharmacology RRMCHAli Veer Ali VeerAinda não há avaliações
- Antiretroviral Agents 2017Documento38 páginasAntiretroviral Agents 2017Iman SaksoukAinda não há avaliações
- Nonsteroidal Anti-Inflammatory Drugs: DR Tarek M Nasrallah Al - AzharDocumento97 páginasNonsteroidal Anti-Inflammatory Drugs: DR Tarek M Nasrallah Al - AzharTarek NasrallahAinda não há avaliações
- Pharmacotherapy of Parkinson's DiseaseDocumento66 páginasPharmacotherapy of Parkinson's DiseaseKenneth NuñezAinda não há avaliações
- Mayra Pagan: Pharmacology-NursingDocumento50 páginasMayra Pagan: Pharmacology-NursingmayraAinda não há avaliações
- Preanesthetic Medication JasminaDocumento44 páginasPreanesthetic Medication Jasminaanjali sAinda não há avaliações
- Antifungal Agent PPT PresentationDocumento38 páginasAntifungal Agent PPT Presentationdinberu tadesseAinda não há avaliações
- Antipyretic DrugsDocumento17 páginasAntipyretic DrugsMuhamad Hafiz Rosli100% (1)
- Antiepileptic DrugsDocumento65 páginasAntiepileptic DrugsZarish IftikharAinda não há avaliações
- Analgesic OintmentDocumento1 páginaAnalgesic OintmentLorenAinda não há avaliações
- AutacoidsDocumento38 páginasAutacoidsdrmayangAinda não há avaliações
- Full Hot TapDocumento91 páginasFull Hot TapHaseeb Bokhari100% (1)
- Morphine (Astramorph)Documento1 páginaMorphine (Astramorph)Adrianne BazoAinda não há avaliações
- Sedative Hypnotic PoisoningDocumento37 páginasSedative Hypnotic PoisoningDeepa WilliamAinda não há avaliações
- (Advances in Nanoscience and Nanotechnology 3) Haghi, A. K. - Zachariah, Ajesh K. - Kalarikkal, Nandakumar - Nanomaterials - Synthesis, Characterization, and Applications-Apple Academic Press (2013)Documento288 páginas(Advances in Nanoscience and Nanotechnology 3) Haghi, A. K. - Zachariah, Ajesh K. - Kalarikkal, Nandakumar - Nanomaterials - Synthesis, Characterization, and Applications-Apple Academic Press (2013)Maman SuperbeAinda não há avaliações
- CH 21Documento32 páginasCH 21Ayyappa SwamyAinda não há avaliações
- B49CE - Tutorial Topic 1 Questions v3Documento2 páginasB49CE - Tutorial Topic 1 Questions v3BuyuAinda não há avaliações
- Adrenergic AntagonistsDocumento23 páginasAdrenergic AntagonistsMirza Shaharyar BaigAinda não há avaliações
- Antiadrenergic DrugsDocumento19 páginasAntiadrenergic DrugsshivanshpandeAinda não há avaliações
- Adrenergic AgonistsDocumento40 páginasAdrenergic AgonistsBenedict Brashi100% (1)
- Central Nervous System Pharmacology: Elly Nurus SakinahDocumento64 páginasCentral Nervous System Pharmacology: Elly Nurus Sakinahkareem92Ainda não há avaliações
- Anxiolytic Sedative-Hypnotic DrugsDocumento31 páginasAnxiolytic Sedative-Hypnotic DrugsRoman MamunAinda não há avaliações
- Cholinergic DrugsDocumento32 páginasCholinergic DrugsApt FianAinda não há avaliações
- Indomethacin 392Documento17 páginasIndomethacin 392Mahadie Hasan JahadAinda não há avaliações
- Antiparkinsons DrugsDocumento19 páginasAntiparkinsons Drugs39 Nayan BhagatAinda não há avaliações
- DiureticsDocumento49 páginasDiureticsamara cheemaAinda não há avaliações
- PhenobarbitalDocumento1 páginaPhenobarbitalJesrel DelotaAinda não há avaliações
- Anterior Pituitary HormonesDocumento46 páginasAnterior Pituitary Hormonespramod bhaleraoAinda não há avaliações
- Anxiolytics, Sedative & Hypnotic DrugsDocumento22 páginasAnxiolytics, Sedative & Hypnotic DrugsPh Hany MohamedAinda não há avaliações
- Pharmacotherapy of AsthmaDocumento53 páginasPharmacotherapy of AsthmaStella Aprilia NurAinda não há avaliações
- Beta-Adrenergic BlockersDocumento14 páginasBeta-Adrenergic BlockersAnonymous NVAWeVWAinda não há avaliações
- Antidiarrheal DrugsDocumento4 páginasAntidiarrheal DrugsNadhirah ZulkifliAinda não há avaliações
- CNS DepressantsDocumento69 páginasCNS DepressantsMicah Lou Calamba100% (1)
- Practical 1-Far 161-FinishDocumento10 páginasPractical 1-Far 161-FinishZulkifli Khairuddin100% (1)
- AntiemeticsDocumento16 páginasAntiemeticswalt65Ainda não há avaliações
- Sem 5/unit-3 Autocoids & Related DrugsDocumento28 páginasSem 5/unit-3 Autocoids & Related DrugsDARSHAN BhirudAinda não há avaliações
- Cholinergic DrugsDocumento29 páginasCholinergic DrugsKiranAinda não há avaliações
- 8B - Antianginal DrugsDocumento70 páginas8B - Antianginal Drugslalitrajindolia100% (1)
- Vidconf Diuretic Antidiuretic 2014Documento51 páginasVidconf Diuretic Antidiuretic 2014naltrisilvianAinda não há avaliações
- IsoprenalineDocumento2 páginasIsoprenalineImmanuel Victor GeorgeAinda não há avaliações
- NEUROPHARMACOLOGYDocumento36 páginasNEUROPHARMACOLOGYDebika DasAinda não há avaliações
- Antidepressants: Depression Is One The Most Treatable Mental IllnessDocumento40 páginasAntidepressants: Depression Is One The Most Treatable Mental IllnessMohammed AbdullahAinda não há avaliações
- Cholinergic Agonists/ Cholinomimetic Agents: Dr. Kyi Kyi Tha Basic Medical Sciences Kulliyyah of Pharmacy IiumDocumento21 páginasCholinergic Agonists/ Cholinomimetic Agents: Dr. Kyi Kyi Tha Basic Medical Sciences Kulliyyah of Pharmacy IiumZhuan AhmadAinda não há avaliações
- Seizure Disorders and Management in Primary Health CareDocumento83 páginasSeizure Disorders and Management in Primary Health CareChidi MbatuegwuAinda não há avaliações
- Preload and AfterloadDocumento28 páginasPreload and Afterloadapi-19916399100% (1)
- Adrenergic AntagonistsDocumento29 páginasAdrenergic AntagonistsBenedict Brashi100% (1)
- Lesson Plan For Brass Band 1Documento2 páginasLesson Plan For Brass Band 1John Benedict VocalesAinda não há avaliações
- DLL Vocales 20th and 21st Century Multimedia FormsDocumento1 páginaDLL Vocales 20th and 21st Century Multimedia FormsJohn Benedict VocalesAinda não há avaliações
- Carnatic Music: Review: Traditional Vocal Music From IndiaDocumento52 páginasCarnatic Music: Review: Traditional Vocal Music From IndiaJohn Benedict VocalesAinda não há avaliações
- A Filtering Mechanism of The Capillaries That Carry Blood To The Brain and Spinal Cord Tissue, Blocking The Passage of Certain SubstancesDocumento1 páginaA Filtering Mechanism of The Capillaries That Carry Blood To The Brain and Spinal Cord Tissue, Blocking The Passage of Certain SubstancesJohn Benedict VocalesAinda não há avaliações
- Reliability and ValidityDocumento23 páginasReliability and ValidityJohn Benedict VocalesAinda não há avaliações
- English 112 Performance TaskDocumento2 páginasEnglish 112 Performance TaskJohn Benedict VocalesAinda não há avaliações
- Unilateral BreathingDocumento3 páginasUnilateral BreathingJohn Benedict VocalesAinda não há avaliações
- Officiating FinalDocumento2 páginasOfficiating FinalJohn Benedict VocalesAinda não há avaliações
- Somethinc-Jakartaxbeauty2023 (Booth XL) (21.12)Documento16 páginasSomethinc-Jakartaxbeauty2023 (Booth XL) (21.12)ARIF WIDIANTORO 211212138Ainda não há avaliações
- Comparing The Degree of Unsaturation of Olive Oil and That of Margarine Jameela Comments by FM PDFDocumento2 páginasComparing The Degree of Unsaturation of Olive Oil and That of Margarine Jameela Comments by FM PDFFrank Massiah0% (1)
- A History of Hindu Chemistry, Chandra Ray, 1903Documento551 páginasA History of Hindu Chemistry, Chandra Ray, 1903Adam TateAinda não há avaliações
- Modeling & Simulation of Water Gas Shift ReactionDocumento5 páginasModeling & Simulation of Water Gas Shift Reactionagarwalashwin32Ainda não há avaliações
- Lab09 Catechol OxidaseDocumento9 páginasLab09 Catechol Oxidaseastromaze10Ainda não há avaliações
- Fill Volume Weight and Other Checks For Parenteral Products During Filling-1Documento4 páginasFill Volume Weight and Other Checks For Parenteral Products During Filling-1SolomonAinda não há avaliações
- Astm A214 PDFDocumento1 páginaAstm A214 PDFgaminAinda não há avaliações
- Salient Features of UFFLDocumento92 páginasSalient Features of UFFLMd. Abu NayeemAinda não há avaliações
- York Fan and CoilDocumento4 páginasYork Fan and CoilPeralta Fco100% (1)
- DC2000C ManualDocumento13 páginasDC2000C ManualThomas WilliamAinda não há avaliações
- VATER Elgate Fence & Gate Systems INFO List JULY19Documento6 páginasVATER Elgate Fence & Gate Systems INFO List JULY19GarryAinda não há avaliações
- Power Generation With Simultaneous Aeration Using A Gravity Vortex TurbineDocumento6 páginasPower Generation With Simultaneous Aeration Using A Gravity Vortex TurbineMunif MoenifAinda não há avaliações
- Turbotak Atomizing Nozzles: Clean Air For IndustryDocumento2 páginasTurbotak Atomizing Nozzles: Clean Air For IndustrytmtoroAinda não há avaliações
- Dust Leaching and Copper CementationDocumento5 páginasDust Leaching and Copper CementationMaysam MohamAinda não há avaliações
- Procare An (TDS)Documento2 páginasProcare An (TDS)liniaxcitoAinda não há avaliações
- Saes G 007Documento5 páginasSaes G 007malika_00Ainda não há avaliações
- Nervous Tissue 1Documento30 páginasNervous Tissue 1OtencianoAinda não há avaliações
- Physical Chemistry For The Life SciencesDocumento1 páginaPhysical Chemistry For The Life SciencessnowblindedAinda não há avaliações
- WKS 8 & 9 - Industrial Dryer 2T 2020-2021Documento26 páginasWKS 8 & 9 - Industrial Dryer 2T 2020-2021Mei Lamfao100% (1)
- F 2129 - 04 - RjixmjkDocumento8 páginasF 2129 - 04 - RjixmjkPrakash MakadiaAinda não há avaliações
- Ball ValvesDocumento112 páginasBall ValvesAlexjohn2009Ainda não há avaliações
- Pidicrrete CF 351.Documento1 páginaPidicrrete CF 351.nickdash09Ainda não há avaliações
- Fermentation in LiebigDocumento8 páginasFermentation in LiebigIngrid Nunes DerossiAinda não há avaliações
- AHU Instalation Manual YorkDocumento36 páginasAHU Instalation Manual YorkBangto Yibsip50% (2)