Você também pode gostar
- Clinical Practice For The Evaluation and Treatment OF Hyperthyroidism and HypothyroidismDocumento69 páginasClinical Practice For The Evaluation and Treatment OF Hyperthyroidism and HypothyroidismTutde SedanaAinda não há avaliações
- Disorders of Thyroid FunctionDocumento83 páginasDisorders of Thyroid FunctionSteven Andriie0% (1)
- Thyroid Function Test: The "Hidden" Health ProblemDocumento34 páginasThyroid Function Test: The "Hidden" Health Problemvjanand07100% (1)
- ThyrotoxicosisDocumento105 páginasThyrotoxicosisAli Murtaza Abbas100% (1)
- Thyroid Function Tests and Goitre SV 24-4-21Documento51 páginasThyroid Function Tests and Goitre SV 24-4-21Lal KhanAinda não há avaliações
- Hypothyroidism in PregnancyDocumento32 páginasHypothyroidism in PregnancyNicks KumarAinda não há avaliações
- Lecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Documento21 páginasLecture 17 - Thyroid Disorders (Including Struma and CA Thyroid) - Dr. M. Robikhul Ikhsan, SP - PD-KEMD (2021)Ivan AditamaAinda não há avaliações
- Hypothyroid in Pregnancy Andi CakraDocumento32 páginasHypothyroid in Pregnancy Andi CakraCakraEkkyAinda não há avaliações
- Endocrinology - 02 (3) - Thyroid Disorders (Courses in Therapeutics and Disease State Management)Documento17 páginasEndocrinology - 02 (3) - Thyroid Disorders (Courses in Therapeutics and Disease State Management)Ali AlyahawiAinda não há avaliações
- Tutorial Presentation: Artika Mala (s170201) Week 2Documento22 páginasTutorial Presentation: Artika Mala (s170201) Week 2Artika MalaAinda não há avaliações
- Thyroid Function Tests: Drneha Mahajan MD PathologyDocumento71 páginasThyroid Function Tests: Drneha Mahajan MD PathologyMukesh Kumar ChaudharyAinda não há avaliações
- Hypothyroidism: Bagian Penyakit Dalam FK Uisu MedanDocumento50 páginasHypothyroidism: Bagian Penyakit Dalam FK Uisu Medanindra saputraAinda não há avaliações
- Class 6 (19.07.2022)Documento70 páginasClass 6 (19.07.2022)Ãqûã FîggâAinda não há avaliações
- Sophie Keyte Bvms (Hons) Mvetmed (Dist) Fhea Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkDocumento24 páginasSophie Keyte Bvms (Hons) Mvetmed (Dist) Fhea Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkStefana UrsuAinda não há avaliações
- Clinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmDocumento73 páginasClinical Approach of Thyroid Disorders: Hypothyroidsm and HyperthyroidsmdiniAinda não há avaliações
- Thyroid Function Tests PPT of IMS BHUDocumento74 páginasThyroid Function Tests PPT of IMS BHUPriyanshu Mandal100% (1)
- Hypothalamic Pitutary Axis and Thyroid Hormone SynthesisDocumento5 páginasHypothalamic Pitutary Axis and Thyroid Hormone Synthesis78 shivangi mauryaAinda não há avaliações
- Thyroid ReportDocumento105 páginasThyroid ReportAARVAinda não há avaliações
- Thyroid Function TestsDocumento24 páginasThyroid Function Testspavani valluriAinda não há avaliações
- Interpretation of Laboratory Thyroid Function Tests: The "Hidden" Health ProblemDocumento38 páginasInterpretation of Laboratory Thyroid Function Tests: The "Hidden" Health Problemalanoud.877Ainda não há avaliações
- CC 3-Lab FKM 17Documento4 páginasCC 3-Lab FKM 17mayabangkurtipotAinda não há avaliações
- FARMAKO Tiroid 2012Documento30 páginasFARMAKO Tiroid 2012Rhandy SeptiantoAinda não há avaliações
- Thyroid Parathyroid (2012)Documento83 páginasThyroid Parathyroid (2012)Hesti AnggrainiAinda não há avaliações
- Thyroiddisease 190216062020Documento42 páginasThyroiddisease 190216062020Manikandan Vp100% (1)
- THYROID Disorders For PB BSCDocumento81 páginasTHYROID Disorders For PB BSCchetankumarbhumireddy50% (2)
- Thyroid Function and Disease: Sponsored by Department of Continuing Medical EducationDocumento69 páginasThyroid Function and Disease: Sponsored by Department of Continuing Medical EducationSriman YarrarapuAinda não há avaliações
- Hypo and Hyperthyroidism 2023Documento113 páginasHypo and Hyperthyroidism 2023Cristina Georgiana SerbanAinda não há avaliações
- Thyroid DiseasesDocumento44 páginasThyroid DiseasesPLDT HOMEAinda não há avaliações
- Hypo and HyperthyroidismDocumento9 páginasHypo and HyperthyroidismChris Opal NamocatcatAinda não há avaliações
- Semen Analysis, Thyroid Function Tests, Renal-2Documento38 páginasSemen Analysis, Thyroid Function Tests, Renal-2deepika bananiAinda não há avaliações
- Thyroid Gland An Diseases of Thyroid D Gland: Omc LectureDocumento59 páginasThyroid Gland An Diseases of Thyroid D Gland: Omc LectureEdward MakemboAinda não há avaliações
- Thiroid DisordersDocumento11 páginasThiroid Disordersرعد النميريAinda não há avaliações
- Thyroid Function: Clinical Chemistry IiiDocumento20 páginasThyroid Function: Clinical Chemistry IiiJannica Dominique ClarosAinda não há avaliações
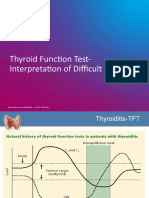
- TFT Interpretation of Difficult CasesDocumento51 páginasTFT Interpretation of Difficult CasesAditya GautamAinda não há avaliações
- Thyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsDocumento7 páginasThyroid Gland L-Thyroxine (T4) Vs Triiodothyronine (T3) : Follicular CellsPrincess Noreen SavellanoAinda não há avaliações
- Thyroid Function TestDocumento28 páginasThyroid Function TestDhinesh Muthusamy100% (1)
- Thyroid Function Tests (TFTS)Documento27 páginasThyroid Function Tests (TFTS)ธิติวุฒิ แสงคล้อยAinda não há avaliações
- 3.thyroid Hormones and DisordersDocumento46 páginas3.thyroid Hormones and DisorderssinayupeAinda não há avaliações
- Thyroid Disorders: Dr. Lubna DwerijDocumento52 páginasThyroid Disorders: Dr. Lubna DwerijNoor MajaliAinda não há avaliações
- Thyroid Talk-FMD RdsDocumento58 páginasThyroid Talk-FMD RdsSriman YarrarapuAinda não há avaliações
- Thyroid GlandDocumento49 páginasThyroid Glandjuliefe pinionAinda não há avaliações
- Disorders of The Thyroid: OutlineDocumento9 páginasDisorders of The Thyroid: OutlineMelissa-Andreea Ardeleanu Carvajal OsorioAinda não há avaliações
- Hypo Thyroid Is MDocumento27 páginasHypo Thyroid Is Mdhiraj parmarAinda não há avaliações
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocumento48 páginasLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteAinda não há avaliações
- HypertyroidismDocumento46 páginasHypertyroidismenriAinda não há avaliações
- Thyroid GlandDocumento9 páginasThyroid GlandZach ReyesAinda não há avaliações
- Hypothyroidism (2016)Documento23 páginasHypothyroidism (2016)Moni RethAinda não há avaliações
- Thyroid Dalam KehamilanDocumento46 páginasThyroid Dalam KehamilanamriAinda não há avaliações
- Hiper Dan Hipotiroid (Revisi)Documento76 páginasHiper Dan Hipotiroid (Revisi)AgusAinda não há avaliações
- Thyroid: Endocrine DiseaseDocumento20 páginasThyroid: Endocrine DiseasehoneymishraAinda não há avaliações
- TIRMODDocumento66 páginasTIRMODYaniAinda não há avaliações
- LEC 04 - Hypo - Hyperthyroidism PDFDocumento115 páginasLEC 04 - Hypo - Hyperthyroidism PDFIoana CozmaAinda não há avaliações
- Thyroid Tests: What Is The Thyroid?Documento8 páginasThyroid Tests: What Is The Thyroid?JyotiAinda não há avaliações
- 3ES-2 Thyroid and Antithyroid Drugs 1436Documento46 páginas3ES-2 Thyroid and Antithyroid Drugs 1436Muath AlqarniAinda não há avaliações
- Thyroid DisordersDocumento55 páginasThyroid DisordersNsubuga Ivan100% (1)
- #30 Thyroid and Thyroid TestingDocumento25 páginas#30 Thyroid and Thyroid TestingasclswisconsinAinda não há avaliações
- MX Thyroid DisordersDocumento52 páginasMX Thyroid Disorderstarakeeshbai1802Ainda não há avaliações
- Thyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!No EverandThyroid Diet: How to improve and cure thyroid disorders, lose weight, and improve metabolism with the help of food!Ainda não há avaliações
- Acute Complication of Diabetes Mellitus: Laksmi SasiariniDocumento43 páginasAcute Complication of Diabetes Mellitus: Laksmi SasiariniClararida RiawanAinda não há avaliações
- Food and Drug InteractionsDocumento4 páginasFood and Drug InteractionsClararida RiawanAinda não há avaliações
- Nfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoDocumento6 páginasNfs Journal: Fangfang Song, Jieun Oh, Kyungwon Lee, Mi Sook ChoClararida RiawanAinda não há avaliações
- Pathophysiology of Muscle Dysfunction in COPDDocumento13 páginasPathophysiology of Muscle Dysfunction in COPDClararida RiawanAinda não há avaliações
- DM 2Documento3 páginasDM 2Clararida RiawanAinda não há avaliações
- Special Nutritional Concerns For The Female Athlete: Kathe A. Gabel, PHD, RD, LDDocumento5 páginasSpecial Nutritional Concerns For The Female Athlete: Kathe A. Gabel, PHD, RD, LDClararida RiawanAinda não há avaliações
- Hand HygieneDocumento3 páginasHand Hygieneashlyn0203Ainda não há avaliações
- Cardiovascular Ultrasound Supervisor/sonographerDocumento4 páginasCardiovascular Ultrasound Supervisor/sonographerapi-121663384Ainda não há avaliações
- Communicable DiseasesDocumento7 páginasCommunicable Diseasesy3nkieAinda não há avaliações
- Acute Bronchitis Chronic Bronchitis: PathophysiologyDocumento2 páginasAcute Bronchitis Chronic Bronchitis: PathophysiologyHarimunsyi Anugerah PratamaAinda não há avaliações
- Ethico Moral Aspects of Nursing 2018Documento50 páginasEthico Moral Aspects of Nursing 2018Zyla De SagunAinda não há avaliações
- An Approach To Young HypertensionDocumento2 páginasAn Approach To Young HypertensionNataShini RajaRatnamAinda não há avaliações
- EM2 - K12 - Renal and Genitourinary System EmergenciesDocumento28 páginasEM2 - K12 - Renal and Genitourinary System EmergenciesrezkadehaAinda não há avaliações
- Endodontics DiagnosisDocumento6 páginasEndodontics DiagnosisRPAinda não há avaliações
- NCP Disturbed Body ImageDocumento5 páginasNCP Disturbed Body ImageAira AlaroAinda não há avaliações
- YeDocumento39 páginasYeRhea RaveloAinda não há avaliações
- Presetation37 MCQDocumento16 páginasPresetation37 MCQBishoy Emile100% (2)
- K14 IPD Dispepsia FungsionalDocumento44 páginasK14 IPD Dispepsia FungsionalenriAinda não há avaliações
- Appendix B:: 2007-2008 NANDA-APPROVED Nursing DiagnosesDocumento1 páginaAppendix B:: 2007-2008 NANDA-APPROVED Nursing DiagnosesKim RamosAinda não há avaliações
- Pediatric OphthalmologyDocumento12 páginasPediatric Ophthalmologyapi-3743483Ainda não há avaliações
- Iptec Teaching LogDocumento2 páginasIptec Teaching Logapi-508924243Ainda não há avaliações
- Nurs FPX 4010 Assessment 1 Collaboration and Leadership Reflection VideoDocumento6 páginasNurs FPX 4010 Assessment 1 Collaboration and Leadership Reflection VideoEmma WatsonAinda não há avaliações
- Medical Surgical NursingDocumento10 páginasMedical Surgical NursingFaye Nervanna Alecha AlferezAinda não há avaliações
- Ambulance Modifiers Table 102015Documento2 páginasAmbulance Modifiers Table 102015Sravan SatheeshAinda não há avaliações
- Filamentary KeratitisDocumento3 páginasFilamentary KeratitisRiski SudaenyAinda não há avaliações
- Prof Qaisar Khan TrialsDocumento56 páginasProf Qaisar Khan TrialsAsim NajamAinda não há avaliações
- Antihistamines For Treating RhinosinusitisDocumento6 páginasAntihistamines For Treating RhinosinusitistopAinda não há avaliações
- CV Fitri DiktiDocumento12 páginasCV Fitri DiktiMilatul AfifahAinda não há avaliações
- Acute Tonsillopharyngitis - Exudative Case Study 2013Documento28 páginasAcute Tonsillopharyngitis - Exudative Case Study 2013YanneBarrido100% (11)
- Assessing TelehealthDocumento10 páginasAssessing TelehealthVINCENT MUHARIAinda não há avaliações
- 5 Processes of LaborDocumento2 páginas5 Processes of LaborElla Rene MartinAinda não há avaliações
- Nursing Bylaws 2009Documento30 páginasNursing Bylaws 2009Silviana FassicaAinda não há avaliações
- Eruptive Xanthoma: A Case Report: Cutis Do NotDocumento4 páginasEruptive Xanthoma: A Case Report: Cutis Do Notbiotech_vidhyaAinda não há avaliações
- Drug Development EssayDocumento5 páginasDrug Development EssayDoyin AwodeleAinda não há avaliações
- Bone Ring Autogenous GraftDocumento4 páginasBone Ring Autogenous GraftHub SciAinda não há avaliações
- Smiles Aug Sep09Documento40 páginasSmiles Aug Sep09Suzana PetreAinda não há avaliações