Você também pode gostar
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- How To Make Your Own PharmacyDocumento27 páginasHow To Make Your Own PharmacyIlyas Pinkhasov100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (894)
- Common Cardiac MedicationsDocumento1 páginaCommon Cardiac MedicationsPaige HardekopfAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
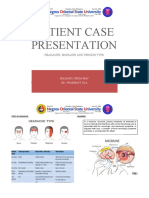
- Patient Case Presentation: Headache: Migraine and Tension TypeDocumento31 páginasPatient Case Presentation: Headache: Migraine and Tension TypeKathleen B Baldado100% (4)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Paida and Lajin Self Healing PDFDocumento10 páginasPaida and Lajin Self Healing PDFMelvin Arvizu100% (1)
- Nursing Practice TestDocumento19 páginasNursing Practice TestEdward Nicko GarciaAinda não há avaliações
- SataDocumento27 páginasSataAkia Cayasan BayaAinda não há avaliações
- Causes, Symptoms and Treatment of Low Blood Pressure (HypotensionDocumento4 páginasCauses, Symptoms and Treatment of Low Blood Pressure (Hypotensionclubsanatate100% (1)
- Hypertension in PregnancyDocumento68 páginasHypertension in PregnancyAbdul MoizAinda não há avaliações
- Optimising HealthDocumento333 páginasOptimising HealthOxygenAinda não há avaliações
- 13-5-2010 MCQ FrcaDocumento79 páginas13-5-2010 MCQ FrcaMohmd Abdulhameed Sayed100% (2)
- Blood Pressure Chart - Normal Blood Pressure RangeDocumento6 páginasBlood Pressure Chart - Normal Blood Pressure RangeKho Cheng KhangAinda não há avaliações
- Drug Study On Emergency DrugsDocumento34 páginasDrug Study On Emergency DrugsMei-mei ZhuangAinda não há avaliações
- Muhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarDocumento54 páginasMuhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarPratiwi PurnamaAinda não há avaliações
- SD causes scaling on sebaceous areasDocumento22 páginasSD causes scaling on sebaceous areasPratiwi PurnamaAinda não há avaliações
- Muhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarDocumento54 páginasMuhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarPratiwi PurnamaAinda não há avaliações
- Muhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarDocumento54 páginasMuhammad Asaad Maidin Departement Microbiology Faculty of Medicine Hasanuddin University, MakassarPratiwi PurnamaAinda não há avaliações
- Yang Et Al 2004 Nicardipine Versus Nitroprusside Infusion As Antihypertensive Therapy in Hypertensive EmergenciesDocumento6 páginasYang Et Al 2004 Nicardipine Versus Nitroprusside Infusion As Antihypertensive Therapy in Hypertensive EmergenciesButyl KamonphunAinda não há avaliações
- Nursing Care Plan for PreeclampsiaDocumento2 páginasNursing Care Plan for PreeclampsiaTsu Wei Chua0% (1)
- Patient Education AssignmentDocumento4 páginasPatient Education Assignmentapi-268670617Ainda não há avaliações
- ROTATION 4 PUTIK HEALTH CENTER TACKLES ALTA PRESYON AND BELLY GUD PROGRAMDocumento11 páginasROTATION 4 PUTIK HEALTH CENTER TACKLES ALTA PRESYON AND BELLY GUD PROGRAMVIERIZA MAE USMAN HAIBERAinda não há avaliações
- Jama Hta ResistenteDocumento9 páginasJama Hta ResistenteMayra Alejandra Prada SerranoAinda não há avaliações
- Jelita Woman PKMDocumento6 páginasJelita Woman PKMIrma Qirani MuhsenAinda não há avaliações
- Medical Abbreviations With Multiple Meanings: A Prescription For DisasterDocumento4 páginasMedical Abbreviations With Multiple Meanings: A Prescription For DisasterNani ReedAinda não há avaliações
- Vox Sanguin Feb 16Documento102 páginasVox Sanguin Feb 16rsdarsono labAinda não há avaliações
- A Study On Assessment of Effect of Samyoga Viruddha Ahara Consumption On Metabolic Syndrome in 35 - 50 Year Old Men and Women of MumbaiDocumento11 páginasA Study On Assessment of Effect of Samyoga Viruddha Ahara Consumption On Metabolic Syndrome in 35 - 50 Year Old Men and Women of MumbaiIJAR JOURNALAinda não há avaliações
- CVD Risk Factors ExplainedDocumento18 páginasCVD Risk Factors ExplainedShin QuinnAinda não há avaliações
- FinalDocumento65 páginasFinalapi-3722454100% (2)
- Hypertensi PDFDocumento10 páginasHypertensi PDFJihan SalsabillaAinda não há avaliações
- Management of Preeclampsia, Severe Preeclampsia, and Eclampsia at Primary Care Facilities in BangladeshDocumento12 páginasManagement of Preeclampsia, Severe Preeclampsia, and Eclampsia at Primary Care Facilities in BangladeshUmi Nur JannahAinda não há avaliações
- SEM-1 EngDocumento2 páginasSEM-1 EngJoko SutantiyoAinda não há avaliações
- Spesialite Obat KardiovaskulerDocumento3 páginasSpesialite Obat Kardiovaskulersumita rahayuAinda não há avaliações
- CBLA (Cardiac Patient)Documento10 páginasCBLA (Cardiac Patient)Llewelyn AgpaoaAinda não há avaliações
- 2 - Antenatal CareDocumento44 páginas2 - Antenatal CareJordanBangot50% (2)
- Inotul Si InimaDocumento8 páginasInotul Si InimaMihail RonnyAinda não há avaliações