Você também pode gostar
- Hypertensive EmergenciesDocumento49 páginasHypertensive EmergenciesSafa Abdualrahaman Ali HamadAinda não há avaliações
- Hypertensive Crisis: Megat Mohd Azman Bin AdzmiDocumento34 páginasHypertensive Crisis: Megat Mohd Azman Bin AdzmiMegat Mohd Azman AdzmiAinda não há avaliações
- Hypertensive Emergencies: BY: Dr. Imtiyaz Hashim (PGR) Dr. Khalida Baloch (Ho)Documento31 páginasHypertensive Emergencies: BY: Dr. Imtiyaz Hashim (PGR) Dr. Khalida Baloch (Ho)امتیاز ہاشم بزنجوAinda não há avaliações
- ICU IV Infusion GuidelinesDocumento2 páginasICU IV Infusion Guidelinessgod34Ainda não há avaliações
- نسخة Infusion rate of emergency drugsDocumento4 páginasنسخة Infusion rate of emergency drugsMohammed FathiAinda não há avaliações
- Intensive Nursing Practicum: SchizophreniaDocumento44 páginasIntensive Nursing Practicum: SchizophreniaAngelicaAinda não há avaliações
- Hypnotics Anxiolytics GuidelinesDocumento28 páginasHypnotics Anxiolytics GuidelinesClarissa YudakusumaAinda não há avaliações
- Oral Pharmacologic Treatment of Type 2 Diabetes Mellitus: A Clinical Practice Guideline Update From The American College of PhysiciansDocumento20 páginasOral Pharmacologic Treatment of Type 2 Diabetes Mellitus: A Clinical Practice Guideline Update From The American College of PhysiciansRoberto López MataAinda não há avaliações
- Computation of Drips: Marla Aurora JacobaDocumento18 páginasComputation of Drips: Marla Aurora JacobaAnne Lorraine Bringas100% (1)
- Criticalcaredrugs 2 PDFDocumento2 páginasCriticalcaredrugs 2 PDFabdallah100% (1)
- KegawatdaruratanDocumento164 páginasKegawatdaruratanmeida astriani gozaziAinda não há avaliações
- Other Sections : Table 1Documento5 páginasOther Sections : Table 1sandeepramanuj4Ainda não há avaliações
- Management of TB-HIV Co-InfectionDocumento17 páginasManagement of TB-HIV Co-InfectionStefanus Raditya PurbaAinda não há avaliações
- CHT DMARDDocumento3 páginasCHT DMARDkoolaberAinda não há avaliações
- Clinical Guideline DepressionDocumento2 páginasClinical Guideline DepressionAllan DiasAinda não há avaliações
- Royal Manchester Children's Hospital - PICU (Version 12.0)Documento2 páginasRoyal Manchester Children's Hospital - PICU (Version 12.0)ibnAinda não há avaliações
- Paediatric Anaesthesia GuideDocumento1 páginaPaediatric Anaesthesia GuideAndrewBeckAinda não há avaliações
- Treatment of Resistant and Refractory HypertensionDocumento21 páginasTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- NOAC ChartDocumento2 páginasNOAC Chartsgod34Ainda não há avaliações
- HT Emergency Final DR Rinelia Minaswary, SPJPDocumento46 páginasHT Emergency Final DR Rinelia Minaswary, SPJPAfdhal MuhammadAinda não há avaliações
- Algorithm - Managing A COPD Exacerbation in Primary CareDocumento1 páginaAlgorithm - Managing A COPD Exacerbation in Primary Caremufidah mawaddahAinda não há avaliações
- DrugsDocumento8 páginasDrugsWinalyn PaderoAinda não há avaliações
- Hypertension LectureDocumento105 páginasHypertension LectureSnigdha GomberAinda não há avaliações
- Pulmonary Edema by DR Gireesh Kumar K PDocumento16 páginasPulmonary Edema by DR Gireesh Kumar K PAETCM Emergency medicineAinda não há avaliações
- Critical Care Drugs 2Documento23 páginasCritical Care Drugs 2Asri Ernadi100% (1)
- Criticalcaredrugs PDFDocumento2 páginasCriticalcaredrugs PDFRakhmat RamadhaniAinda não há avaliações
- Classification, Epidemiology, Pathophysiology of HypertensionDocumento35 páginasClassification, Epidemiology, Pathophysiology of Hypertensionastrid abrahamsAinda não há avaliações
- Standard Treatment GuidelinesDocumento5 páginasStandard Treatment Guidelinesbournvilleeater100% (1)
- Chest & Abdominal X-Ray Interpretation: LT Col NK Jain GD SPL (Radiology) MH JabalpurDocumento116 páginasChest & Abdominal X-Ray Interpretation: LT Col NK Jain GD SPL (Radiology) MH JabalpurabolojeenAinda não há avaliações
- USMLE 1 Hematology BookDocumento368 páginasUSMLE 1 Hematology BookPRINCEAinda não há avaliações
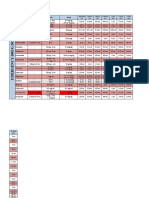
- Drug Dilution Conc. Dose: Newborn 3KG 1 Month 4KG 3 Month 5KG 6 Month 8KG 1 Year 10KG 3 Years 15KG 5 Years 18KGDocumento2 páginasDrug Dilution Conc. Dose: Newborn 3KG 1 Month 4KG 3 Month 5KG 6 Month 8KG 1 Year 10KG 3 Years 15KG 5 Years 18KGAngeline FanardyAinda não há avaliações
- PocketGuide FINAL6 PDFDocumento2 páginasPocketGuide FINAL6 PDFSolomon Seth SallforsAinda não há avaliações
- Pass 2010 ScheduleDocumento1 páginaPass 2010 SchedulewldcrdAinda não há avaliações
- Antiarrhythmic Drugs 1Documento32 páginasAntiarrhythmic Drugs 1AliImadAlKhasakiAinda não há avaliações
- Simple Method of Acid Base Balance InterpretationDocumento3 páginasSimple Method of Acid Base Balance InterpretationShawn McMahonAinda não há avaliações
- Management of Severe Hypertension, Hypertension in Special ConditionDocumento43 páginasManagement of Severe Hypertension, Hypertension in Special Conditionabhandlung100% (3)
- HCSW - Holistic Care and Assessment in Primary CareDocumento1 páginaHCSW - Holistic Care and Assessment in Primary CaregireeshsachinAinda não há avaliações
- Noradrenaline Infusion Rate BSUH Critical CareDocumento4 páginasNoradrenaline Infusion Rate BSUH Critical CareAndreiCostei100% (1)
- Essential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 2 PDFDocumento1 páginaEssential ENT by Rogan J Corbridge MB BS, BSC, 2nd Ed 2011 2 PDFMariam Qais100% (1)
- Poster 10 PALS 01 01 ENG V20100927 PDFDocumento1 páginaPoster 10 PALS 01 01 ENG V20100927 PDFAndy XiaoAinda não há avaliações
- Pro32 SupraventricularTachycardiaDocumento1 páginaPro32 SupraventricularTachycardiaRonald KendallAinda não há avaliações
- Legacy Effect in Diabetes MnanagementDocumento9 páginasLegacy Effect in Diabetes MnanagementSouradipta GangulyAinda não há avaliações
- Surgery 2012Documento28 páginasSurgery 2012max_21ruAinda não há avaliações
- Adrenergic Receptor ChartDocumento1 páginaAdrenergic Receptor Chartsas345sas345Ainda não há avaliações
- Know Common Disease ManagementDocumento14 páginasKnow Common Disease Managementcdx25Ainda não há avaliações
- E - Cart DrugsDocumento18 páginasE - Cart Drugs'SheenMarkReal'100% (2)
- Medications Used in Code Blue EmergenciesDocumento24 páginasMedications Used in Code Blue EmergenciesAhmed Ali Mohammed AlbashirAinda não há avaliações
- Notes For Clincal CasesDocumento12 páginasNotes For Clincal CasesMandeepAinda não há avaliações
- Acute Myocardial Infarction by DR Gireesh Kumar K PDocumento18 páginasAcute Myocardial Infarction by DR Gireesh Kumar K PAETCM Emergency medicine50% (2)
- Chan, Johnson - TreatmentGuidelines PDFDocumento0 páginaChan, Johnson - TreatmentGuidelines PDFBogdan CarabasAinda não há avaliações
- Antibiotic Dosing Guidelines For Renal ImpairmentDocumento6 páginasAntibiotic Dosing Guidelines For Renal ImpairmentvitauxianaAinda não há avaliações
- Immunosuppressant Drugs Drug Name Class Function Method/Receptor UseDocumento3 páginasImmunosuppressant Drugs Drug Name Class Function Method/Receptor UseKristin DouglasAinda não há avaliações
- EKG Interpretation: Amir Aziz AlkatiriDocumento51 páginasEKG Interpretation: Amir Aziz AlkatiriShabrina Sari MedinaAinda não há avaliações
- Common TreatmentsDocumento5 páginasCommon TreatmentsRaj MandumulaAinda não há avaliações
- 1.1. Krisis Hipertensi - Dr. Saugi AbduhDocumento29 páginas1.1. Krisis Hipertensi - Dr. Saugi AbduhdmaulidaAinda não há avaliações
- Idiopathic Thrombocytopenic Purpura (ITP) or Immune ThrombocytopeniaDocumento11 páginasIdiopathic Thrombocytopenic Purpura (ITP) or Immune ThrombocytopeniaSreekrishnan TrikkurAinda não há avaliações
- Glucose Specific Gravity BUN Serum Creatinine LDH Protein Albumin Bilirubin Total Cholesterol Triglyceride Uric Acid CPKDocumento4 páginasGlucose Specific Gravity BUN Serum Creatinine LDH Protein Albumin Bilirubin Total Cholesterol Triglyceride Uric Acid CPKPanJan BalAinda não há avaliações
- ACLS TeoriDocumento27 páginasACLS TeoriTita Luthfia100% (1)
- Hypertensive CrisesDocumento42 páginasHypertensive Crisescabinetuldeigiena0% (2)
- DAFTAR PUSTAKA FiksDocumento1 páginaDAFTAR PUSTAKA FiksagustinaAinda não há avaliações
- Varicella: Case ReportDocumento2 páginasVaricella: Case ReportagustinaAinda não há avaliações
- Varicella: Case ReportDocumento1 páginaVaricella: Case ReportagustinaAinda não há avaliações
- Case Report: Identity of PatientDocumento7 páginasCase Report: Identity of PatientagustinaAinda não há avaliações
- Lead Time BiasDocumento1 páginaLead Time BiasEvi LoAinda não há avaliações
- Aromatherapy - Overvew, Safety and Quality IssuesDocumento6 páginasAromatherapy - Overvew, Safety and Quality IssuesMBAinda não há avaliações
- HypertensionDocumento13 páginasHypertensionAbigail BascoAinda não há avaliações
- Child AbuseDocumento10 páginasChild Abusejadeyjade100% (1)
- Neonatal PneumoniaDocumento15 páginasNeonatal Pneumoniaapi-19916399Ainda não há avaliações
- Medical Surgical Nursing Nclex questionsGI1Documento11 páginasMedical Surgical Nursing Nclex questionsGI1dee_day_8100% (2)
- Annex Pil DHCPDocumento11 páginasAnnex Pil DHCPAbdelrahman MohamedAinda não há avaliações
- Professionals and Practitioners in CounselingDocumento20 páginasProfessionals and Practitioners in CounselingJac KieAinda não há avaliações
- MetaanalysisDocumento12 páginasMetaanalysisAhmed BadrAinda não há avaliações
- Chapter 15 - Obsessive-Ompulsive and Related DisordersDocumento7 páginasChapter 15 - Obsessive-Ompulsive and Related Disordersmyer pasandalanAinda não há avaliações
- CP 2Documento24 páginasCP 2Bandameedi RamuAinda não há avaliações
- Fractured Root Tips During Dental Extractions and Retained Root Fragments. A Clinical Dilemma?Documento7 páginasFractured Root Tips During Dental Extractions and Retained Root Fragments. A Clinical Dilemma?DrAshish KalawatAinda não há avaliações
- Functional Medicine Coaching PDFDocumento142 páginasFunctional Medicine Coaching PDFAnabell Garcia100% (13)
- Toward A Unified Treatment For Emotional Disorders - Barlow Et. AlDocumento26 páginasToward A Unified Treatment For Emotional Disorders - Barlow Et. AlpoopmanAinda não há avaliações
- Plab Mock TestsDocumento17 páginasPlab Mock TestsMisbah ShahzadiAinda não há avaliações
- Lanoxin: (Digoxin) InjectionDocumento35 páginasLanoxin: (Digoxin) InjectionZainAinda não há avaliações
- VITAMIN K Drug StudyDocumento2 páginasVITAMIN K Drug StudyMarl DumiligAinda não há avaliações
- Soft Scrub DIA 00375Documento6 páginasSoft Scrub DIA 00375Victor LopezAinda não há avaliações
- Abdominal Aortic Aneurysmn FINAL WORDDocumento16 páginasAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasAinda não há avaliações
- Pain Management in Endodontics PDFDocumento6 páginasPain Management in Endodontics PDFdavid bbAinda não há avaliações
- Alliant Health SystemDocumento3 páginasAlliant Health Systemmuhammadk_107Ainda não há avaliações
- Lecture Notes Surgery in Pregnancy Dr. BonleonDocumento5 páginasLecture Notes Surgery in Pregnancy Dr. BonleonMonica Dianne AdtoonAinda não há avaliações
- Rev 1 Final Pembicara IDI Edit BackgroundDocumento80 páginasRev 1 Final Pembicara IDI Edit BackgroundYandasru BogorAinda não há avaliações
- Career Research ProjectDocumento11 páginasCareer Research Projectapi-497927045Ainda não há avaliações
- Rife Morris FishbeinDocumento9 páginasRife Morris FishbeinuncoveringconsciousAinda não há avaliações
- For Printing Grand Case Group1Documento37 páginasFor Printing Grand Case Group1Joco Bordeos AripAinda não há avaliações
- 5 IV CannulationDocumento61 páginas5 IV CannulationNursing Superintendent (SH)Ainda não há avaliações
- CTP MP Plumbing Code PDFDocumento29 páginasCTP MP Plumbing Code PDFVALIENT CANCERANAinda não há avaliações
- Blood CancerDocumento20 páginasBlood Cancernuman ijazAinda não há avaliações
- The Druggists General Receipt BookDocumento518 páginasThe Druggists General Receipt BookSawyer_Books100% (1)