Você também pode gostar
- Health Teaching Plan For Dengue Hemorrhagic FeverDocumento3 páginasHealth Teaching Plan For Dengue Hemorrhagic Fevershiramu100% (5)
- Pre-Op Case Protocol #4Documento2 páginasPre-Op Case Protocol #4IC BAinda não há avaliações
- Hematology Cell Morphology ChartDocumento2 páginasHematology Cell Morphology ChartMiaoAinda não há avaliações
- 27 Tumor OvariumDocumento44 páginas27 Tumor OvariumJulius KingAinda não há avaliações
- UrooncologyDocumento49 páginasUrooncologyanwar jabariAinda não há avaliações
- Colon Cancer:: Pfizer Headquarter Office. Wednesday 18/02/2015Documento92 páginasColon Cancer:: Pfizer Headquarter Office. Wednesday 18/02/2015José Mauricio PeñalozaAinda não há avaliações
- FTPDocumento5 páginasFTPHaya RihanAinda não há avaliações
- HCC PresentationDocumento37 páginasHCC PresentationnagdadAinda não há avaliações
- CyberKnife SBRT - High Accuracy For High Control of Moving TargetsDocumento48 páginasCyberKnife SBRT - High Accuracy For High Control of Moving TargetsRicardo MejíasAinda não há avaliações
- Clinical Oncology AssignmentDocumento11 páginasClinical Oncology Assignmentapi-632146706Ainda não há avaliações
- Journal of Surgical Oncology - 2010 - Huh - Preoperative Carcinoembryonic Antigen Level As An Independent Prognostic FactorDocumento5 páginasJournal of Surgical Oncology - 2010 - Huh - Preoperative Carcinoembryonic Antigen Level As An Independent Prognostic Factorfathul rachmanAinda não há avaliações
- Tumor TestisDocumento30 páginasTumor TestisYunita ElfiaAinda não há avaliações
- NMSC Excision Margins AuditDocumento36 páginasNMSC Excision Margins AuditnuwanrajapakshaAinda não há avaliações
- For Hepatocellular Carcinoma: Living Donor Liver TransplantationDocumento46 páginasFor Hepatocellular Carcinoma: Living Donor Liver TransplantationtasarimkutusuAinda não há avaliações
- Major Liver Resection PIN IKABDI Bali 4 Okt 2014 711DFDocumento32 páginasMajor Liver Resection PIN IKABDI Bali 4 Okt 2014 711DFElandha PutriAinda não há avaliações
- NCIN Colorectal Survival DatabriefingDocumento2 páginasNCIN Colorectal Survival DatabriefingMilo ZabálAinda não há avaliações
- 0850 Adam MED BdImYaK YG - OipkDocumento66 páginas0850 Adam MED BdImYaK YG - OipkFlaviusAinda não há avaliações
- Hall A DR Devilla Apasl Sirt Talk1 Luncheon PDFDocumento45 páginasHall A DR Devilla Apasl Sirt Talk1 Luncheon PDFMarlon Dela CruzAinda não há avaliações
- NMSC Excision Margins AuditDocumento36 páginasNMSC Excision Margins AuditnuwanrajapakshaAinda não há avaliações
- 361 Full PDFDocumento5 páginas361 Full PDFgrigmihAinda não há avaliações
- Chemotherapy and Targeting Therapy in Colon CancerDocumento62 páginasChemotherapy and Targeting Therapy in Colon CancerIndonesian Journal of CancerAinda não há avaliações
- Male/Female Ratio:: Spindle Cell Lipomatous LesionsDocumento10 páginasMale/Female Ratio:: Spindle Cell Lipomatous LesionsMuhammad ZainAinda não há avaliações
- Bladder Cancer - Daniel LeeDocumento110 páginasBladder Cancer - Daniel LeePhan Quốc ThọAinda não há avaliações
- Esophageal Carcinoma: Mark Louie M. Lanting, MDDocumento44 páginasEsophageal Carcinoma: Mark Louie M. Lanting, MDlouie10279098Ainda não há avaliações
- V5 - Bladder Cancer Survey'24 - FinalDocumento12 páginasV5 - Bladder Cancer Survey'24 - FinaldhirajmocindiaAinda não há avaliações
- Barb Melo SkyDocumento17 páginasBarb Melo SkyAfiqah So JasmiAinda não há avaliações
- The Emergence of Liver Transplantation For Hilar CholangiocarcinomaDocumento109 páginasThe Emergence of Liver Transplantation For Hilar CholangiocarcinomatasarimkutusuAinda não há avaliações
- La Eficacia de Los Biomarcadores de Muerte Celular en Suero para Diagnosticar El Cáncer Del Tracto BiliarDocumento7 páginasLa Eficacia de Los Biomarcadores de Muerte Celular en Suero para Diagnosticar El Cáncer Del Tracto BiliarNicolás MateoJrAinda não há avaliações
- Hepatocellular CarcinomaDocumento62 páginasHepatocellular CarcinomaWilliams Emmanuel AdeyeyeAinda não há avaliações
- CT Scan in Woman Oncology GynecologyDocumento109 páginasCT Scan in Woman Oncology GynecologyAstien SuzmanAinda não há avaliações
- Optimizing The Management of NSCLCDocumento34 páginasOptimizing The Management of NSCLCANISA RACHMITA ARIANTI 2020Ainda não há avaliações
- Huh Et Al-2010-Journal of Surgical OncologyDocumento5 páginasHuh Et Al-2010-Journal of Surgical OncologyFieska AzizahAinda não há avaliações
- Nerve-Sparing Laparoscopic Radical Cystectomy Technique and Initial OutcomesDocumento6 páginasNerve-Sparing Laparoscopic Radical Cystectomy Technique and Initial Outcomes肖楚天Ainda não há avaliações
- Work-Up and Management of Lung CancerDocumento90 páginasWork-Up and Management of Lung Cancerrsbahia100% (2)
- Small Cell Lung Cancer (SCLC) and Tkis in NSCLCDocumento73 páginasSmall Cell Lung Cancer (SCLC) and Tkis in NSCLCAgi Azhari SandiniAinda não há avaliações
- TACE Colon CaDocumento25 páginasTACE Colon CaHaider RabeeAinda não há avaliações
- SC 2009118Documento5 páginasSC 2009118Yanne LewerissaAinda não há avaliações
- 2023.06 TACT Interim Five Year OutcomesDocumento8 páginas2023.06 TACT Interim Five Year OutcomesRichard PhillipsAinda não há avaliações
- CaRectum (DR - Soetamto Wibowo)Documento25 páginasCaRectum (DR - Soetamto Wibowo)Elandha Putri100% (1)
- Fix JurnalDocumento12 páginasFix JurnalYolanda Qonita ShalihatAinda não há avaliações
- Clinicaloncologyassignment JosephspencerDocumento10 páginasClinicaloncologyassignment Josephspencerapi-633248237Ainda não há avaliações
- Articol Extenso 2Documento4 páginasArticol Extenso 2David CalinAinda não há avaliações
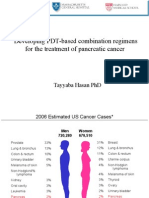
- Developing PDT-based Combination Regimens For The Treatment of Pancreatic CancerDocumento33 páginasDeveloping PDT-based Combination Regimens For The Treatment of Pancreatic CancerFirdosh DekhaiyaAinda não há avaliações
- A Gynecology Oncology Group/NRG Oncology Study: Presented By: Daniela Matei, MDDocumento18 páginasA Gynecology Oncology Group/NRG Oncology Study: Presented By: Daniela Matei, MDJorge AvilaAinda não há avaliações
- Implementsi PMK 8-2015 PPRADocumento47 páginasImplementsi PMK 8-2015 PPRAMaya DamanikAinda não há avaliações
- Nakamura 2015Documento6 páginasNakamura 2015pakemainmainAinda não há avaliações
- HepatomaDocumento33 páginasHepatomaRozen RyuhaAinda não há avaliações
- Circulating Tumor Cells (Dr. Minetta Liu)Documento34 páginasCirculating Tumor Cells (Dr. Minetta Liu)National Press FoundationAinda não há avaliações
- Charles Catton, Brian O'Sullivan, Robert Dinniwell, Anthony Griffin, Peter C Ferguson, Rebecca Gladdy, David Mccready, Martin Blackstein, Abha Gupta, Lisa W Le, Peter ChungDocumento15 páginasCharles Catton, Brian O'Sullivan, Robert Dinniwell, Anthony Griffin, Peter C Ferguson, Rebecca Gladdy, David Mccready, Martin Blackstein, Abha Gupta, Lisa W Le, Peter ChungRida Anita YunikawatiAinda não há avaliações
- Breast Unit - University Malaya Medical CentreDocumento47 páginasBreast Unit - University Malaya Medical CentreIndonesian Journal of CancerAinda não há avaliações
- He Pa To Cellular CarcinomaDocumento16 páginasHe Pa To Cellular CarcinomaArdiestya Dias S.Ainda não há avaliações
- D105 APBI Future - My Point of ViewDocumento70 páginasD105 APBI Future - My Point of ViewSoc. Portuguesa de Radioterapia OncologiaAinda não há avaliações
- Penanganan Lesi Pra Kanker Serviks: I Nyoman Bayu MahendraDocumento76 páginasPenanganan Lesi Pra Kanker Serviks: I Nyoman Bayu MahendraHandy PutraAinda não há avaliações
- Final Onc Paper 1Documento13 páginasFinal Onc Paper 1api-645453685Ainda não há avaliações
- CHEN DimDocumento68 páginasCHEN DimDiana Alexandra Pacheco TorresAinda não há avaliações
- Akses Hemodialisis Yang Optimal Berdasarkan Perspektif Nefrologis (Webinar B.TKV 5 Sept 2020) (Edited)Documento39 páginasAkses Hemodialisis Yang Optimal Berdasarkan Perspektif Nefrologis (Webinar B.TKV 5 Sept 2020) (Edited)puji kristiniAinda não há avaliações
- Metabolomics of Colorectal Cancer in MalaysiaDocumento22 páginasMetabolomics of Colorectal Cancer in MalaysiaMrShippingFreeAinda não há avaliações
- Journal 1 - Multidetector Computed Tomography in The Evaluation of Gastric Malignancy A Multicenteric StudyDocumento6 páginasJournal 1 - Multidetector Computed Tomography in The Evaluation of Gastric Malignancy A Multicenteric StudypasyaAinda não há avaliações
- Bevakalp 07Documento10 páginasBevakalp 07Er Prajakta TiwariAinda não há avaliações
- All CANCERDocumento40 páginasAll CANCERKaren Joyce Costales MagtanongAinda não há avaliações
- Colorectal Cancer: Diagnosis and Clinical ManagementNo EverandColorectal Cancer: Diagnosis and Clinical ManagementJohn H. ScholefieldAinda não há avaliações
- Management of Urologic Cancer: Focal Therapy and Tissue PreservationNo EverandManagement of Urologic Cancer: Focal Therapy and Tissue PreservationAinda não há avaliações
- Fast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesNo EverandFast Facts: Cholangiocarcinoma: Diagnostic and therapeutic advances are improving outcomesAinda não há avaliações
- Spence 2017Documento5 páginasSpence 2017Afkar30Ainda não há avaliações
- Primary 5D Home Based Learning Time Table: Form (FR)Documento3 páginasPrimary 5D Home Based Learning Time Table: Form (FR)Afkar30Ainda não há avaliações
- Dok Baru 2021-06-07 08.38.01Documento3 páginasDok Baru 2021-06-07 08.38.01Afkar30Ainda não há avaliações
- Dok Baru 2021-06-07 08.38.01 - 1Documento1 páginaDok Baru 2021-06-07 08.38.01 - 1Afkar30Ainda não há avaliações
- Gallstone Disease and The Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Observational StudiesDocumento7 páginasGallstone Disease and The Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Observational StudiesAfkar30Ainda não há avaliações
- Outcomes of Endoscopic Ultrasound-Guided Biliary Drainage: A Systematic Review and Meta-AnalysisDocumento9 páginasOutcomes of Endoscopic Ultrasound-Guided Biliary Drainage: A Systematic Review and Meta-AnalysisAfkar30Ainda não há avaliações
- Dok Baru 2021-06-07 08.38.01 - 2Documento1 páginaDok Baru 2021-06-07 08.38.01 - 2Afkar30Ainda não há avaliações
- FS PustakaDocumento4 páginasFS PustakaAfkar30Ainda não há avaliações
- Prospective Clinical Study: Mass Closure Versus Layer Closure of Abdominal WallDocumento6 páginasProspective Clinical Study: Mass Closure Versus Layer Closure of Abdominal WallAfkar30Ainda não há avaliações
- 03 Chemo PrincDocumento17 páginas03 Chemo PrincMareeze HattaAinda não há avaliações
- Original Research Paper: GastroenterologyDocumento3 páginasOriginal Research Paper: GastroenterologyAfkar30Ainda não há avaliações
- Guidelines For Surgery in The HIV Patient: Samuel Smit, MB CHB, M Med (Surg)Documento8 páginasGuidelines For Surgery in The HIV Patient: Samuel Smit, MB CHB, M Med (Surg)Afkar30Ainda não há avaliações
- DR Kiki Lukman Patofisiologi Acute CholangitisDocumento36 páginasDR Kiki Lukman Patofisiologi Acute CholangitisAfkar30Ainda não há avaliações
- Abstrak Jonata (English)Documento1 páginaAbstrak Jonata (English)Afkar30Ainda não há avaliações
- Salah Satu Syarat Guna Memperoleh Gelar Dokter Spesialis BedahDocumento1 páginaSalah Satu Syarat Guna Memperoleh Gelar Dokter Spesialis BedahAfkar30Ainda não há avaliações
- Imaging Correlation of The Degree of Degenerative L4-5 Spondylolisthesis With The Corresponding Amount of Facet FluidDocumento6 páginasImaging Correlation of The Degree of Degenerative L4-5 Spondylolisthesis With The Corresponding Amount of Facet FluidAfkar30Ainda não há avaliações
- Appendicial MassDocumento2 páginasAppendicial MassAfkar30Ainda não há avaliações
- Appendicial MassDocumento2 páginasAppendicial MassAfkar30Ainda não há avaliações
- POster Mba Alicia JugaDocumento23 páginasPOster Mba Alicia JugaAfkar30Ainda não há avaliações
- Appendicial MassDocumento15 páginasAppendicial MassAfkar30Ainda não há avaliações
- Announcement BSS GP PDFDocumento2 páginasAnnouncement BSS GP PDFAfkar30Ainda não há avaliações
- Abstrak Dr. Deny SafitriDocumento2 páginasAbstrak Dr. Deny SafitriAfkar30Ainda não há avaliações
- Abstrak Jonata (English)Documento1 páginaAbstrak Jonata (English)Afkar30Ainda não há avaliações
- Abstrak Jonata (English)Documento1 páginaAbstrak Jonata (English)Afkar30Ainda não há avaliações
- KoreksiDocumento6 páginasKoreksiAfkar30Ainda não há avaliações
- Trauma Buli Dan UrethraDocumento6 páginasTrauma Buli Dan UrethraAfkar30Ainda não há avaliações
- Esofageal Stenosis - DR AnungDocumento26 páginasEsofageal Stenosis - DR AnungAfkar30Ainda não há avaliações
- Blunt Abdominal Trauma PDFDocumento6 páginasBlunt Abdominal Trauma PDFrizkaAinda não há avaliações
- Abses Hepar 2014Documento2 páginasAbses Hepar 2014Afkar30Ainda não há avaliações
- What Kate Did at WorkDocumento3 páginasWhat Kate Did at WorkSpeech & Language Therapy in PracticeAinda não há avaliações
- Glossopharyngeal Nerve Injury Following Tonsillectomy 5542Documento4 páginasGlossopharyngeal Nerve Injury Following Tonsillectomy 5542Kenza SeddikAinda não há avaliações
- StaphylococcusDocumento28 páginasStaphylococcusAliyah SajaAinda não há avaliações
- Med-Surg Lecture 4th Year 1st Sem (Incomplete)Documento70 páginasMed-Surg Lecture 4th Year 1st Sem (Incomplete)Raezhell Dianne RachoAinda não há avaliações
- 10 Chemical Tests Fecal Occult BloodDocumento11 páginas10 Chemical Tests Fecal Occult BloodAdarshBijapurAinda não há avaliações
- ESR Microsed PermaiDocumento20 páginasESR Microsed PermaiHishamudin RaisAinda não há avaliações
- Coronavirus Disease (COVID-19) Pandemic: EditorialDocumento3 páginasCoronavirus Disease (COVID-19) Pandemic: EditorialBeb HaqAinda não há avaliações
- Association of Multi-Drug Resistant Bacteria With Sanitation of Street Vendors FoodDocumento14 páginasAssociation of Multi-Drug Resistant Bacteria With Sanitation of Street Vendors FoodMamta AgarwalAinda não há avaliações
- Saddle BlockDocumento3 páginasSaddle BlockVasu DevanAinda não há avaliações
- The Prevalence of Depression and Anxiety in Iranian Patients With Diabetes Mellitus: A Systematic Review and Meta-AnalysisDocumento11 páginasThe Prevalence of Depression and Anxiety in Iranian Patients With Diabetes Mellitus: A Systematic Review and Meta-Analysisselamat parminAinda não há avaliações
- Acoustic NeuromaDocumento19 páginasAcoustic NeuromaIshAinda não há avaliações
- The Cardiovascular SystemDocumento43 páginasThe Cardiovascular Systemtravis efraimAinda não há avaliações
- Zoonotic Diseases - Laboratory RabbitsDocumento2 páginasZoonotic Diseases - Laboratory RabbitsramperoughAinda não há avaliações
- Treatment Plan Form John Doe - Coun755Documento3 páginasTreatment Plan Form John Doe - Coun755api-310813184Ainda não há avaliações
- Makerere AR 67th Graduation Day2 22ndfeb2017Documento40 páginasMakerere AR 67th Graduation Day2 22ndfeb2017The Independent Magazine100% (2)
- MCQDocumento6 páginasMCQalirbidiAinda não há avaliações
- Jurnal Pengaruh Musik Mozart Terhadap Perubahan Perilaku Hiperaktif Anak Adhd Usia 7-12 TahunDocumento16 páginasJurnal Pengaruh Musik Mozart Terhadap Perubahan Perilaku Hiperaktif Anak Adhd Usia 7-12 TahunroryputrisartikaAinda não há avaliações
- Primary Review: Psoas Abscess: Case of The LiteratureDocumento3 páginasPrimary Review: Psoas Abscess: Case of The LiteratureDung Tran HoangAinda não há avaliações
- MTQ0OTY0ODkyNA PDFDocumento2 páginasMTQ0OTY0ODkyNA PDFHansa BorichaAinda não há avaliações
- Ciesluk Meagan Cover LetterDocumento1 páginaCiesluk Meagan Cover Letterapi-508459908Ainda não há avaliações
- Mental DisorderDocumento18 páginasMental DisorderMaria Gabriela GimenezAinda não há avaliações
- B. Physical Fitness (Skill-Related Fitness) : (No. of Hits)Documento1 páginaB. Physical Fitness (Skill-Related Fitness) : (No. of Hits)Oikawa MinamahalAinda não há avaliações
- Palicka Simpozion Management RiscDocumento60 páginasPalicka Simpozion Management Risccornelialautarescu6411Ainda não há avaliações
- Government College of Nursing JodhpurDocumento7 páginasGovernment College of Nursing JodhpurNaresh JeengarAinda não há avaliações
- K-02 (Imunologi Dasar)Documento40 páginasK-02 (Imunologi Dasar)amiksalamahAinda não há avaliações
- Stabilis-Monographie-Doxorubicin Hydrochloride Liposome PegDocumento9 páginasStabilis-Monographie-Doxorubicin Hydrochloride Liposome PegSepti Marta SariAinda não há avaliações
- Pricelist 13 Juli 2020Documento21 páginasPricelist 13 Juli 2020Achmad Sya'idAinda não há avaliações