Você também pode gostar
- Lower Is Better - FinalDocumento91 páginasLower Is Better - FinalJamsidul Hassan RajibAinda não há avaliações
- Lower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsDocumento59 páginasLower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsJamsidul Hassan RajibAinda não há avaliações
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Documento51 páginas2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserAinda não há avaliações
- Intensity of Cholesterol Lowering With Statin in PatientsDocumento23 páginasIntensity of Cholesterol Lowering With Statin in Patientsandri ansyahAinda não há avaliações
- PSAP 2019 Dyslipidemia PDFDocumento24 páginasPSAP 2019 Dyslipidemia PDFdellykets_323822919Ainda não há avaliações
- PSAP 2019 Dyslipidemia PDFDocumento24 páginasPSAP 2019 Dyslipidemia PDFdellykets_323822919Ainda não há avaliações
- HIPERLIPIDEMIADocumento10 páginasHIPERLIPIDEMIAMarianaAinda não há avaliações
- Understanding The Needs of The High Productive DyslipidemiaDocumento47 páginasUnderstanding The Needs of The High Productive DyslipidemiachchchchkAinda não há avaliações
- LipidsupdateDocumento23 páginasLipidsupdatedrshekarforyouAinda não há avaliações
- A Pragmatic View of The New Cholesterol Treatment GuidelinesDocumento4 páginasA Pragmatic View of The New Cholesterol Treatment GuidelinesMaria Fernanda CoralAinda não há avaliações
- ATP IV HandoutDocumento2 páginasATP IV Handouthafidzz1Ainda não há avaliações
- Virta HealthDocumento18 páginasVirta Healthismail100% (1)
- Lipids Topic DiscussionDocumento10 páginasLipids Topic Discussionapi-665372449Ainda não há avaliações
- Dyslipidemia ATP4 GUIDLINESDocumento9 páginasDyslipidemia ATP4 GUIDLINESSandy GunawanAinda não há avaliações
- Guidelines DyslipidDocumento49 páginasGuidelines Dyslipidnoveldycb89Ainda não há avaliações
- 2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3Documento15 páginas2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3CoolrobertizAinda não há avaliações
- Screening and Management of Lipids: Patient Population: ObjectiveDocumento20 páginasScreening and Management of Lipids: Patient Population: ObjectiveKatie Kroll BradyAinda não há avaliações
- Beyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDocumento54 páginasBeyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDilan GalaryAinda não há avaliações
- Management of Blood Cholesterol 2019Documento2 páginasManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassAinda não há avaliações
- Global Risk of Cardiovascular Disease: Assessment and ApplicationDocumento18 páginasGlobal Risk of Cardiovascular Disease: Assessment and ApplicationEmdan SengadjiAinda não há avaliações
- NACHC Statin Guideline Snapshot GenericDocumento14 páginasNACHC Statin Guideline Snapshot GenericSaad KhanAinda não há avaliações
- Dyslipidaemia 2019Documento61 páginasDyslipidaemia 2019fatima.shqeratAinda não há avaliações
- Role of Rosuvastatin in The Treatment of DyslipidemiaDocumento16 páginasRole of Rosuvastatin in The Treatment of DyslipidemiaabcdefAinda não há avaliações
- What's New in Lipid GuidelinesDocumento31 páginasWhat's New in Lipid GuidelinesYunita WidyaningsihAinda não há avaliações
- HyperlipidemiaDocumento38 páginasHyperlipidemiaAadhan ArveeAinda não há avaliações
- 2017 DCP 1. Telmisartan Untuk KasusDocumento26 páginas2017 DCP 1. Telmisartan Untuk KasusOcto IndradjajaAinda não há avaliações
- Slide Speaker Candesartan For Hypertension in CKD PatientsDocumento43 páginasSlide Speaker Candesartan For Hypertension in CKD Patientsesdras pramuditaAinda não há avaliações
- Pharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyDocumento37 páginasPharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyKevin JiaAinda não há avaliações
- Nicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorDocumento5 páginasNicotinic Acid 10-20% 10-20% 14-35% 30-70% Reasonable To PoorvmvlivAinda não há avaliações
- Causes & Prevention of Coronary Artery DiseaseDocumento41 páginasCauses & Prevention of Coronary Artery DiseaseeenagpurcongAinda não há avaliações
- Management of Dyslipidemia and The Prevention of Cardiovascular DiseaseDocumento2 páginasManagement of Dyslipidemia and The Prevention of Cardiovascular DiseaseBenny TrisaktyariAinda não há avaliações
- Dyslipidemia - 2Documento17 páginasDyslipidemia - 2Mohamed AbouzaidAinda não há avaliações
- JNC 8 PDFDocumento15 páginasJNC 8 PDFcut herlindaAinda não há avaliações
- 10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDocumento3 páginas10-Year Risk of Fatal CVD Is Based On Risk Factors: Age, Smoking, Sex, Systolic Blood Pressure and Total CholesterolDidik SiswandoroAinda não há avaliações
- 2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsDocumento37 páginas2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsIman SaksoukAinda não há avaliações
- Dr. Endah Dewati K.S. SPJPDocumento41 páginasDr. Endah Dewati K.S. SPJPbudiantoAinda não há avaliações
- 2018 Cholesterol Guidelines Made Simple ToolDocumento22 páginas2018 Cholesterol Guidelines Made Simple ToolLeoberto Batista Pereira SobrinhoAinda não há avaliações
- Guidelines Made Simple Tool 2018 CholesterolDocumento22 páginasGuidelines Made Simple Tool 2018 CholesterolHussain HameedAinda não há avaliações
- Safety and Efficacy of Statin TherapyDocumento13 páginasSafety and Efficacy of Statin TherapyAlexa ArceAinda não há avaliações
- Drogas en Dislipidemia para Prevemncion CVDocumento19 páginasDrogas en Dislipidemia para Prevemncion CVeleanhy95Ainda não há avaliações
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocumento8 páginasRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارAinda não há avaliações
- Atherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineDocumento21 páginasAtherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineHeryanti PusparisaAinda não há avaliações
- Ascvd PrimaryDocumento21 páginasAscvd Primaryprk prkAinda não há avaliações
- Guidelines Made Simple Tool 2018 CholesterolDocumento22 páginasGuidelines Made Simple Tool 2018 CholesterolMuhammad Ali Ridho ShahabAinda não há avaliações
- Cholesterol Guidelines Review 2020Documento6 páginasCholesterol Guidelines Review 2020oriannaocantoAinda não há avaliações
- Pharmacotherapy of HypertensionDocumento90 páginasPharmacotherapy of HypertensionJambo BuneAinda não há avaliações
- New Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesDocumento6 páginasNew Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesJustinaAinda não há avaliações
- Statin Therapyforthe PreventionaDocumento15 páginasStatin Therapyforthe PreventionaMr XAinda não há avaliações
- Hyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services UniversityDocumento58 páginasHyperlipidemia: Brian V. Reamy, MD, Colonel, USAF, MC Chair - Department of Family Medicine Uniformed Services Universityayloleh87Ainda não há avaliações
- Diabetes Mellitus: Geriatrics Evaluation & ManagementDocumento4 páginasDiabetes Mellitus: Geriatrics Evaluation & ManagementAngeles SlzrAinda não há avaliações
- Farmakologi Sindrom Metablik CitraDocumento63 páginasFarmakologi Sindrom Metablik CitraAnonymous UaWvUXL6L1Ainda não há avaliações
- Statin 150324032853 Conversion Gate01Documento24 páginasStatin 150324032853 Conversion Gate01magdAinda não há avaliações
- Baseline Low-Density LipoproteinDocumento9 páginasBaseline Low-Density LipoproteinjoAinda não há avaliações
- Guidelines Made Simple Tool 2018 CholesterolDocumento22 páginasGuidelines Made Simple Tool 2018 CholesterolSafira HalimatussadiahAinda não há avaliações
- Ongoing Therapy and MonitoringDocumento1 páginaOngoing Therapy and MonitoringDaveMartoneAinda não há avaliações
- 2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryDocumento77 páginas2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryBetsy Brown ByersmithAinda não há avaliações
- 2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/ Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummaryDocumento77 páginas2018 Aha/Acc/Aacvpr/Aapa/Abc/Acpm/Ada/Ags/ Apha/Aspc/Nla/Pcna Guideline On The Management of Blood Cholesterol: Executive SummarydanielAinda não há avaliações
- Lipid ManagementDocumento2 páginasLipid ManagementMedicina FamiliarAinda não há avaliações
- International Business, 14e (Daniels, Et Al) - Chapter 05Documento26 páginasInternational Business, 14e (Daniels, Et Al) - Chapter 05Jeffrey MillingerAinda não há avaliações
- M Scan BrochureDocumento8 páginasM Scan BrochureM-ScanAinda não há avaliações
- Year 9 QM1 - Drugs EducationDocumento2 páginasYear 9 QM1 - Drugs EducationDavid WilliamsAinda não há avaliações
- Lagochilascar Ecuador 98Documento2 páginasLagochilascar Ecuador 98MaikellSegoviaAinda não há avaliações
- Hand in Glove-The Burma Army and The Drug Trade in Shan StateDocumento64 páginasHand in Glove-The Burma Army and The Drug Trade in Shan StatePugh JuttaAinda não há avaliações
- Bactericidal Activity of Flavonoids Isolated From Muntingia CalaburaDocumento7 páginasBactericidal Activity of Flavonoids Isolated From Muntingia CalaburaSSR-IIJLS JournalAinda não há avaliações
- Acetylsalicylic AcidDocumento13 páginasAcetylsalicylic AcidMuhammad Tariq Khan100% (1)
- Intranasal Steroids in PediatricsDocumento39 páginasIntranasal Steroids in PediatricsKishore ChandkiAinda não há avaliações
- California Retailers Guide To Hazardous Waste ComplianceDocumento4 páginasCalifornia Retailers Guide To Hazardous Waste ComplianceStericycle100% (1)
- High Risk Medication PolicyDocumento44 páginasHigh Risk Medication PolicyDewi Ratna SariAinda não há avaliações
- 1.1. Nanotechnology: Nanotechnology Is The Science and Technology at Nano Scale, Which Ranges About 1-100Documento22 páginas1.1. Nanotechnology: Nanotechnology Is The Science and Technology at Nano Scale, Which Ranges About 1-100Subham BoseAinda não há avaliações
- BuscopanDocumento2 páginasBuscopancen janber cabrillosAinda não há avaliações
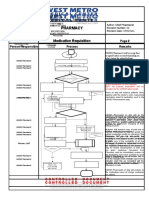
- Pharmacy Pharmacy: Medication Requisition Medication RequisitionDocumento1 páginaPharmacy Pharmacy: Medication Requisition Medication RequisitionSharie Grace ImlanAinda não há avaliações
- ALPRAZOLAMDocumento13 páginasALPRAZOLAMAishiteru Mawarna B LaAinda não há avaliações
- Mega Investor Presentation 4q2018Documento47 páginasMega Investor Presentation 4q2018hau vuvanAinda não há avaliações
- Public Assessment Report Decentralised ProcedureDocumento26 páginasPublic Assessment Report Decentralised Procedurefad12345Ainda não há avaliações
- Bio WorldDocumento198 páginasBio Worldmc_goaAinda não há avaliações
- Qsar by Hansch Analysis: Faculty of Pharmaceutical Sciences, Maharshi Dayanand University, RohtakDocumento5 páginasQsar by Hansch Analysis: Faculty of Pharmaceutical Sciences, Maharshi Dayanand University, RohtakastrimentariAinda não há avaliações
- PT Pis: Deskripsi Barang Harga SatuanDocumento42 páginasPT Pis: Deskripsi Barang Harga SatuanAndi MufidahAinda não há avaliações
- Commercial Considerations of Drug Discovery ProgramDocumento549 páginasCommercial Considerations of Drug Discovery ProgramparinitaAinda não há avaliações
- Plethico Pharmaceuticals Limited, Kalaria, Indore Plethico Pharmaceuticals Limited, Kalaria, IndoreDocumento22 páginasPlethico Pharmaceuticals Limited, Kalaria, Indore Plethico Pharmaceuticals Limited, Kalaria, IndoreGarimaAinda não há avaliações
- Encapsulation Technologies:: A General OverviewDocumento21 páginasEncapsulation Technologies:: A General OverviewZorica Knežević-JugovićAinda não há avaliações
- Nutra Plus ProductsDocumento82 páginasNutra Plus ProductssavaninikunjdAinda não há avaliações
- OPPI Guidelines On Good Laboratory Practices (GLP)Documento31 páginasOPPI Guidelines On Good Laboratory Practices (GLP)Vitalis MbuyaAinda não há avaliações
- LevemirDocumento36 páginasLevemirsigitAinda não há avaliações
- ChemotherapyDocumento102 páginasChemotherapyJoseph John K Pothanikat100% (1)
- Validation of A Method For The Quantitation of Mdma in Seized Materials by Spectrophotometric MethodDocumento6 páginasValidation of A Method For The Quantitation of Mdma in Seized Materials by Spectrophotometric MethodalbertuAinda não há avaliações
- Gaba HPLCDocumento8 páginasGaba HPLCsisnaingaungAinda não há avaliações
- Nozinan 2013Documento6 páginasNozinan 2013Tom StAinda não há avaliações
- 8th Sem SyllabusDocumento29 páginas8th Sem SyllabusDeemay AdmazAinda não há avaliações