Você também pode gostar
- Case Study of Liver CirrhosisDocumento3 páginasCase Study of Liver Cirrhosisbuzz Q100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Case Study of AmoebiasisDocumento7 páginasCase Study of Amoebiasisbuzz Q75% (4)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Case Study of LeptospirosisDocumento4 páginasCase Study of Leptospirosisbuzz Q75% (4)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Case Study of DMDocumento6 páginasCase Study of DMbuzz Q0% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Case Study of AsthmaDocumento6 páginasCase Study of Asthmabuzz Q100% (4)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- GUT3Documento143 páginasGUT3buzz Q100% (1)
- ReadmeDocumento1 páginaReadmebuzz QAinda não há avaliações
- Musical InstrumentsDocumento12 páginasMusical Instrumentsbuzz QAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
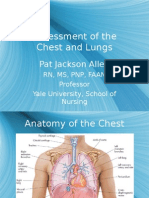
- Assessment of The Chest and Lungs: Pat Jackson AllenDocumento50 páginasAssessment of The Chest and Lungs: Pat Jackson Allenbuzz Q100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Assessment of The Skin: Pat Jackson AllenDocumento104 páginasAssessment of The Skin: Pat Jackson Allenbuzz Q100% (5)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- NeurologyDocumento42 páginasNeurologybuzz Q100% (2)
- UrologyDocumento28 páginasUrologybuzz QAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Care of The NewbornDocumento5 páginasCare of The Newbornbuzz Q100% (2)
- Growth and DevelopmentDocumento6 páginasGrowth and Developmentbuzz Q100% (3)
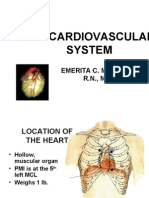
- The Cardiovascular SystemDocumento20 páginasThe Cardiovascular Systembuzz QAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Lesson 1 Human Breathing SystemDocumento37 páginasLesson 1 Human Breathing SystemDavid Lawrence GarciaAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Effects of Yoga On Digestive SystemDocumento54 páginasEffects of Yoga On Digestive SystemManish Nahar33% (3)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- PPP Anatomy of Endocrine SystemDocumento23 páginasPPP Anatomy of Endocrine SystemMarisol AcostaAinda não há avaliações
- Heart Failure Differential DiagnosesDocumento3 páginasHeart Failure Differential DiagnosesAizel ManiagoAinda não há avaliações
- Defense Mechanisms of The BodyDocumento33 páginasDefense Mechanisms of The Bodymazna khalilAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Obstructive UropathyDocumento14 páginasObstructive Uropathyanwar jabariAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- Development of Nervous SystemDocumento71 páginasDevelopment of Nervous SystemAbdimalik AliAinda não há avaliações
- Revalence of Thyroid Disorders in A Tertiary Care CenterDocumento5 páginasRevalence of Thyroid Disorders in A Tertiary Care CenterAvisa Cetta CresmaAinda não há avaliações
- BiologicalBasisBehavior Bluestone PDFDocumento30 páginasBiologicalBasisBehavior Bluestone PDFdaphnereezeAinda não há avaliações
- Acute Pulmonary Edema - NEJMDocumento4 páginasAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- The Heart Is A Muscle: BloodDocumento8 páginasThe Heart Is A Muscle: BloodJhoewil QuintuaAinda não há avaliações
- Summary of Nervous SystemDocumento4 páginasSummary of Nervous SystemDerel PatriaAinda não há avaliações
- Sense OrgansDocumento8 páginasSense OrgansKeelah BennAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Endocrine System Transes PDFDocumento5 páginasEndocrine System Transes PDFShemess ButgorgAinda não há avaliações
- Life Processes PDFDocumento12 páginasLife Processes PDFSankalp MouryaAinda não há avaliações
- Marieb ch3dDocumento20 páginasMarieb ch3dapi-229554503Ainda não há avaliações
- PGY 451 2009 Exam 1 With AnswersDocumento6 páginasPGY 451 2009 Exam 1 With AnswersJackson FoxAinda não há avaliações
- Pancreatic PathologyDocumento7 páginasPancreatic Pathologyzeroun24100% (1)
- Tissues - McqsDocumento5 páginasTissues - McqsDocumentSharerAinda não há avaliações
- Case StudyDocumento10 páginasCase StudyJib SinsuatAinda não há avaliações
- Development Urinary SystemDocumento33 páginasDevelopment Urinary Systempavi7muruganathan75% (4)
- Excretion Question AnsweredDocumento9 páginasExcretion Question AnsweredKeelah BennAinda não há avaliações
- Physiology of Autonomic Nervous System: J J M Medical College, Davangere. Dept of AnesthesiaDocumento117 páginasPhysiology of Autonomic Nervous System: J J M Medical College, Davangere. Dept of AnesthesiaKithminaAinda não há avaliações
- Unlq6073 PDFDocumento8 páginasUnlq6073 PDFSrinu VijayaAinda não há avaliações
- Hubungan Kepercayaan Diri Dengan Pola Pemberian Air Susu Ibu Pada Ibu Menyusui Yang BekerjaDocumento7 páginasHubungan Kepercayaan Diri Dengan Pola Pemberian Air Susu Ibu Pada Ibu Menyusui Yang BekerjaamilyapraditaAinda não há avaliações
- Hydrocephalus PathophysiologyDocumento3 páginasHydrocephalus PathophysiologyErika CadawanAinda não há avaliações
- Nursing NotesDocumento6 páginasNursing NotesAngel CauilanAinda não há avaliações
- DLP - Human SkinDocumento3 páginasDLP - Human SkinIrene Anastasia100% (1)
- The Stucture of The HeartDocumento3 páginasThe Stucture of The Heartkamran imtiazAinda não há avaliações