Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- 10 1016@j Ijscr 2020 01 020Documento4 páginas10 1016@j Ijscr 2020 01 020ari naAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Omphalocele and Gastroschisis: Wendy Nguyen and Kumar BelaniDocumento8 páginasOmphalocele and Gastroschisis: Wendy Nguyen and Kumar Belaniari naAinda não há avaliações
- Primary Umbilical Endometriosis. Case Report and Discussion On Management OptionsDocumento7 páginasPrimary Umbilical Endometriosis. Case Report and Discussion On Management Optionsari naAinda não há avaliações
- The Efficacy of Crown Rump Length Measurement by Ultrasound in Estimating The Gestational AgeDocumento7 páginasThe Efficacy of Crown Rump Length Measurement by Ultrasound in Estimating The Gestational Ageari naAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- 1 s2.0 S0959804911009336 MainDocumento11 páginas1 s2.0 S0959804911009336 Mainari naAinda não há avaliações
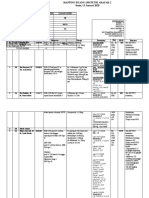
- Mapping Ruang Obstetri Arafah 2 Sabtu, 11 Januari 2020Documento5 páginasMapping Ruang Obstetri Arafah 2 Sabtu, 11 Januari 2020ari naAinda não há avaliações
- S S I L I: Eptic Hock After Ntracervical Aminaria NsertionDocumento3 páginasS S I L I: Eptic Hock After Ntracervical Aminaria Nsertionari naAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Keterangan Hamil: 0 Post Sc:5 Post Pv:0 Post Vakum ILO:0 Post Manual Plasenta:0 Pasien Ginekologi:0 Post Kuretase: 1Documento3 páginasKeterangan Hamil: 0 Post Sc:5 Post Pv:0 Post Vakum ILO:0 Post Manual Plasenta:0 Pasien Ginekologi:0 Post Kuretase: 1ari naAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Keterangan Hamil: 0 Post Sc:5 Post Pv:0 Post Vakum ILO:0 Post Manual Plasenta:0 Pasien Ginekologi:0 Post Kuretase: 1Documento3 páginasKeterangan Hamil: 0 Post Sc:5 Post Pv:0 Post Vakum ILO:0 Post Manual Plasenta:0 Pasien Ginekologi:0 Post Kuretase: 1ari naAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Best Practice & Research Clinical Obstetrics and GynaecologyDocumento13 páginasBest Practice & Research Clinical Obstetrics and Gynaecologyari naAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Gestational Diabetes: By: Fatima ChoudaryDocumento26 páginasGestational Diabetes: By: Fatima Choudaryari naAinda não há avaliações
- MATERNAL DISEASE-PEB-EclampsiaDocumento10 páginasMATERNAL DISEASE-PEB-Eclampsiaari naAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Agnes Lee Thrombosis PresentationDocumento37 páginasAgnes Lee Thrombosis Presentationari naAinda não há avaliações
- Slide Obgyn Jurnal ReadingDocumento18 páginasSlide Obgyn Jurnal Readingari naAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Preeklampsia NEJMDocumento10 páginasPreeklampsia NEJMari naAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Options For Questions 1-4Documento6 páginasOptions For Questions 1-4ari naAinda não há avaliações
- Obstetric William Prenatal DiganosisDocumento7 páginasObstetric William Prenatal Diganosisari naAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Case Report AIMS IMAMDocumento2 páginasCase Report AIMS IMAMari naAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Wound Healing Mila-YesyDocumento18 páginasWound Healing Mila-Yesyari naAinda não há avaliações
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Breakout Obgyn - DR Azen PDFDocumento44 páginasBreakout Obgyn - DR Azen PDFarie susantoAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Comparative Study of Micronised Progesterone Versus ISOXSUPRINE IN THE PREVENTION OF PRETERM LABOURDocumento7 páginasComparative Study of Micronised Progesterone Versus ISOXSUPRINE IN THE PREVENTION OF PRETERM LABOURshivareddychAinda não há avaliações
- Medical Report BHS InggrisDocumento15 páginasMedical Report BHS InggrisSyifa asqafAinda não há avaliações
- 20 Questions On ObDocumento5 páginas20 Questions On ObCes Espino TorreAinda não há avaliações
- Inter-Hospital Variations in Labor Induction and OutcomesDocumento9 páginasInter-Hospital Variations in Labor Induction and OutcomesStéphanieAinda não há avaliações
- MisoprostolDocumento7 páginasMisoprostolSava1988Ainda não há avaliações
- Daftar Pustaka ObgynDocumento1 páginaDaftar Pustaka ObgynISMJAinda não há avaliações
- 2b - Antenatal Check Up History TakingDocumento16 páginas2b - Antenatal Check Up History TakingAnudeep DeekondaAinda não há avaliações
- Antenatal CareDocumento33 páginasAntenatal CareKamran Afzal100% (1)
- Contoh PDF Bakso KudaDocumento20 páginasContoh PDF Bakso KudaNuken Rochmadiah ApriantiAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Antepartum & Postpartum Hemorrhage (APH &PPH) : Anita DeodharDocumento81 páginasAntepartum & Postpartum Hemorrhage (APH &PPH) : Anita DeodharAnjali Rahul AjmeriAinda não há avaliações
- Partograph Exercise: Case 1Documento2 páginasPartograph Exercise: Case 1Madhusmita Nayak100% (1)
- Using Doula Care As A Complement To NFPDocumento9 páginasUsing Doula Care As A Complement To NFPpkmAinda não há avaliações
- Task 1 Gestational DisorderDocumento2 páginasTask 1 Gestational DisorderSherlocknovAinda não há avaliações
- Tugas Analisa Jurnal Mahasiswa s1 KebidananDocumento10 páginasTugas Analisa Jurnal Mahasiswa s1 Kebidananridani 13Ainda não há avaliações
- Twins: SupervisorDocumento10 páginasTwins: Supervisorكيرلس مجدىAinda não há avaliações
- Presented By: Balancar, Robert Jimenez, Jay Lebumfacil, Lani PearlDocumento30 páginasPresented By: Balancar, Robert Jimenez, Jay Lebumfacil, Lani PearlAnonymous fGyJwzxTAinda não há avaliações
- Introduction To OBGDocumento23 páginasIntroduction To OBGsindhujojo100% (1)
- Journal 4Documento5 páginasJournal 4nana nurdahliaAinda não há avaliações
- Roisin Ryan Obstetrics Final Year RevisionDocumento78 páginasRoisin Ryan Obstetrics Final Year RevisionDanny SchAinda não há avaliações
- SBS - Birth Doula Training InfoDocumento4 páginasSBS - Birth Doula Training InfoNicole Niscala SchwartzAinda não há avaliações
- VersionDocumento15 páginasVersionAnees Siddiqui100% (1)
- Management of Spontaneous Abortion - American Family PhysicianDocumento8 páginasManagement of Spontaneous Abortion - American Family PhysicianGwEn LimAinda não há avaliações
- 1.antepartum HeamorrhageDocumento26 páginas1.antepartum Heamorrhagems khanAinda não há avaliações
- Obstetric Emergency and Anesthetic ManagementDocumento11 páginasObstetric Emergency and Anesthetic ManagementmichaelAinda não há avaliações
- Cardio To C OgraphyDocumento6 páginasCardio To C OgraphyChinedu H. DuruAinda não há avaliações
- No Kode ICD Diagnosa: 10 Besar Penyakit Terbanyak Pasien Rawat Inap 2019Documento6 páginasNo Kode ICD Diagnosa: 10 Besar Penyakit Terbanyak Pasien Rawat Inap 2019wedayani nitiAinda não há avaliações
- OET Writing Task - Nikki GrantDocumento4 páginasOET Writing Task - Nikki Grantgodeva17Ainda não há avaliações
- Heifers and Multiparous Cows Are Affected by Dystocia and Its Implications On The Viability of The PregnancyDocumento5 páginasHeifers and Multiparous Cows Are Affected by Dystocia and Its Implications On The Viability of The PregnancyIndah frysay marbunAinda não há avaliações
- MCN 209 Obgyne Rotation: Postpartum HemorrhageDocumento10 páginasMCN 209 Obgyne Rotation: Postpartum HemorrhageMonique LeonardoAinda não há avaliações
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNo EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeAinda não há avaliações
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNo EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouAinda não há avaliações
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeNo EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeNota: 3.5 de 5 estrelas3.5/5 (13)