Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- SCOLIOSISDocumento4 páginasSCOLIOSISapi-3822433Ainda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- 1 Polypharmacy Facts and FiguresDocumento10 páginas1 Polypharmacy Facts and Figuresghostanime2002Ainda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- NAPLEX Drugs TableDocumento71 páginasNAPLEX Drugs Tablestarobin100% (3)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Jo Spences Camera Therapy Personal Therapeutic PhotographyDocumento15 páginasJo Spences Camera Therapy Personal Therapeutic PhotographytatikamiAinda não há avaliações
- Nur 3112 Spring2014 Multisystem Case StudyDocumento7 páginasNur 3112 Spring2014 Multisystem Case Studyapi-277274156100% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- MastoiditisDocumento37 páginasMastoiditisAkanksha EkkaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- RCT Appraisal Sheets 2005 English-2Documento4 páginasRCT Appraisal Sheets 2005 English-2Mahardhika AcintyaAinda não há avaliações
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- GloballSurgery ICN907166 PDFDocumento10 páginasGloballSurgery ICN907166 PDFKian GonzagaAinda não há avaliações
- Health Screenig ServicesDocumento36 páginasHealth Screenig ServicesTarachand LalwaniAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
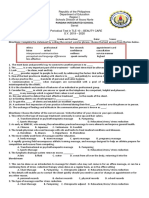
- 1st Periodical Test in Beauty Care 10 - Wellness MasssageDocumento2 páginas1st Periodical Test in Beauty Care 10 - Wellness MasssageBelinda Lapsit100% (5)
- ErickkkkDocumento19 páginasErickkkkMOULIANNA8949Ainda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Review of Related Literatures and Studies LLLLDocumento17 páginasReview of Related Literatures and Studies LLLLreynald salva95% (19)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Thyroid StormDocumento11 páginasThyroid StormAndrew UtamaAinda não há avaliações
- Osteochondritis Dissecans - OrthoInfo - AAOSDocumento5 páginasOsteochondritis Dissecans - OrthoInfo - AAOSDita Ambarsari SyafruddinAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Secondary Arterial HypertensionDocumento32 páginasSecondary Arterial HypertensionAndi SusiloAinda não há avaliações
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- PriceDocumento27 páginasPriceBugar Wahyu PAinda não há avaliações
- COR PULMONALE - MahasiswaDocumento14 páginasCOR PULMONALE - MahasiswaGalih Maygananda PutraAinda não há avaliações
- Reflex Testing Methods FOR Evaluating CNS Development: Charles C. Thomas PublisherDocumento55 páginasReflex Testing Methods FOR Evaluating CNS Development: Charles C. Thomas PublisherDeborah Salinas100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Final Literautre ReviewDocumento4 páginasFinal Literautre Reviewapi-549231596Ainda não há avaliações
- Sexual DisordersDocumento5 páginasSexual DisordersJerry100% (1)
- Sexual EnergyDocumento1 páginaSexual EnergykukutxiAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- NCLEX Exam Obstetrical Nursing - Antepartum (50 Items)Documento13 páginasNCLEX Exam Obstetrical Nursing - Antepartum (50 Items)Catherine Manalo100% (1)
- Anna Ostaszewska - Scientific Researches On Christian PsychotherapyDocumento23 páginasAnna Ostaszewska - Scientific Researches On Christian Psychotherapysad1410Ainda não há avaliações
- Breast Cancer ProtocolDocumento24 páginasBreast Cancer Protocolsilveo100% (1)
- Pricelist TreatmentDocumento2 páginasPricelist TreatmentikaAinda não há avaliações
- Second Announcement Sunshine 2019Documento20 páginasSecond Announcement Sunshine 2019alvinAinda não há avaliações
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Autogenic TrainingDocumento2 páginasAutogenic TrainingAleena ThakurtaAinda não há avaliações
- ValiumDocumento1 páginaValiumKatie McPeekAinda não há avaliações
- Portable Devices Used For Home Testing in Obstructive Sleep ApneaDocumento42 páginasPortable Devices Used For Home Testing in Obstructive Sleep ApneaCalifornia Technology Assessment Forum0% (1)
- Ansel's Pharmaceutical DosageDocumento8 páginasAnsel's Pharmaceutical DosageChandra FatmaAinda não há avaliações