Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Hoarseness and Laryngopharyngeal RefluxDocumento5 páginasHoarseness and Laryngopharyngeal RefluxThitamhrnAinda não há avaliações
- HypertensionDocumento52 páginasHypertensionpatriciajesikaAinda não há avaliações
- Pemicu 1 Endokrin MargaretDocumento60 páginasPemicu 1 Endokrin MargaretThitamhrnAinda não há avaliações
- Recap MR02-041118A: AlbertDocumento5 páginasRecap MR02-041118A: AlbertThitamhrnAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Health History QuestionnaireDocumento3 páginasHealth History QuestionnairejlaferriereAinda não há avaliações
- Traditional indian medicine.அகஸ்தியர் சித்த வைத்திய நிலையம் - AGASTHIAR ALL DIESEACESDocumento26 páginasTraditional indian medicine.அகஸ்தியர் சித்த வைத்திய நிலையம் - AGASTHIAR ALL DIESEACESDeebaAinda não há avaliações
- AMC Clinical Recalls 2019 (COMPLETE TILL JUL) - SponsoredDocumento46 páginasAMC Clinical Recalls 2019 (COMPLETE TILL JUL) - SponsoredIgor Dias67% (3)
- Introduction To Oral Pathology 1Documento32 páginasIntroduction To Oral Pathology 1Hoor M TahanAinda não há avaliações
- DM, DKA, and IDMDocumento19 páginasDM, DKA, and IDMJennyu YuAinda não há avaliações
- Vol 27.5 - Neurocritical Care.2021Documento363 páginasVol 27.5 - Neurocritical Care.2021RafaelAinda não há avaliações
- Hema 1 ErythropoiesisDocumento20 páginasHema 1 Erythropoiesismarie judimor gomezAinda não há avaliações
- Peds Ati ReviewDocumento32 páginasPeds Ati ReviewMorgan100% (41)
- English Robot Script FinalDocumento4 páginasEnglish Robot Script FinalKumaresh MuthuAinda não há avaliações
- High-Risk Newborns and Child During Illness and Hospitalization - Pediatric NursingDocumento200 páginasHigh-Risk Newborns and Child During Illness and Hospitalization - Pediatric Nursingjaggermeister20100% (8)
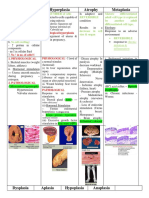
- Hypertrophy Hyperplasia Atrophy MetaplasiaDocumento20 páginasHypertrophy Hyperplasia Atrophy MetaplasiaYunQingTanAinda não há avaliações
- Muscle Weakness in Adults PDFDocumento14 páginasMuscle Weakness in Adults PDFJames TianAinda não há avaliações
- Cardiac Function Tests Anatomy of The HeartDocumento8 páginasCardiac Function Tests Anatomy of The HeartJosiah BimabamAinda não há avaliações
- Infecciones Necrotizantes de Tejidos Blandos TheLancet 2023Documento14 páginasInfecciones Necrotizantes de Tejidos Blandos TheLancet 2023Nicolás LaverdeAinda não há avaliações
- 2012 Mrcog 1 RecallsDocumento17 páginas2012 Mrcog 1 RecallsMahavir GemavatAinda não há avaliações
- Icd 10 CodeDocumento3 páginasIcd 10 Codecheryll duenasAinda não há avaliações
- Lichen Striatus Successfully Treated With Photodynamic TherapyDocumento3 páginasLichen Striatus Successfully Treated With Photodynamic TherapyOzheanAMAinda não há avaliações
- Common Symptoms of Gastrointestinal and Abdominal DiseaseDocumento34 páginasCommon Symptoms of Gastrointestinal and Abdominal DiseaseMalueth AnguiAinda não há avaliações
- Neuro UrologyDocumento53 páginasNeuro UrologymoominjunaidAinda não há avaliações
- Case Study GonorrheaDocumento19 páginasCase Study GonorrheaErika ThereseAinda não há avaliações
- 93 - 08 Bantar 7 Hal 306-312Documento7 páginas93 - 08 Bantar 7 Hal 306-312amilyapraditaAinda não há avaliações
- Systemic Inflammatory Response Syndrome The CurrenDocumento6 páginasSystemic Inflammatory Response Syndrome The CurrenberlianAinda não há avaliações
- Adult Referral For PC Assessment FormDocumento1 páginaAdult Referral For PC Assessment Formwhy u reading thisAinda não há avaliações
- Clinico-Radiological Profile in Covid - 19 PatientsDocumento6 páginasClinico-Radiological Profile in Covid - 19 PatientsInternational Journal of Innovative Science and Research Technology100% (1)
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorDocumento2 páginasStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaAinda não há avaliações
- Dental Pulse 12th Ed - PhysiologyDocumento107 páginasDental Pulse 12th Ed - PhysiologyLangAinda não há avaliações
- Rife FrequenciesDocumento471 páginasRife Frequencieslopans100% (9)
- Moving Exam NCM 109 Lecture For PrintDocumento6 páginasMoving Exam NCM 109 Lecture For PrintMoneto CasaganAinda não há avaliações
- Cerebral Salt Wasting Syndrome - StatPearls - NCBI BookshelfDocumento4 páginasCerebral Salt Wasting Syndrome - StatPearls - NCBI BookshelfOnggo WiliyantoAinda não há avaliações
- Sistema Curativo Por Dieta Amucosa - Arnold Ehret - WWW - Arnoldehret.infoDocumento8 páginasSistema Curativo Por Dieta Amucosa - Arnold Ehret - WWW - Arnoldehret.infoLorena CalahorroAinda não há avaliações