Você também pode gostar
- ACLS DrugsDocumento4 páginasACLS DrugsEduard Espeso Chiong-Gandul Jr.Ainda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Presentation Syntax Score TCT 2008 PDFDocumento33 páginasPresentation Syntax Score TCT 2008 PDFElla MihAinda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- Update ACLSDocumento64 páginasUpdate ACLSVenansius Ratno KurniawanAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- NTSB LIRR ReportDocumento26 páginasNTSB LIRR ReportNewsdayAinda não há avaliações
- Pendidikan Pasien Cath LabDocumento10 páginasPendidikan Pasien Cath LabAgnesthesiaAinda não há avaliações
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Medical Abbreviations Used by Hospital ProfessionalsDocumento27 páginasMedical Abbreviations Used by Hospital ProfessionalsunforeverAinda não há avaliações
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- SMS Result and Data 2021Documento161 páginasSMS Result and Data 2021ChinaAinda não há avaliações
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- J Clinic Periodontology - 2023 - Herrera - Association Between Periodontal Diseases and Cardiovascular Diseases DiabetesDocumento23 páginasJ Clinic Periodontology - 2023 - Herrera - Association Between Periodontal Diseases and Cardiovascular Diseases DiabetesPablo González CalviñoAinda não há avaliações
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Presented by DR Rahul D AgrawalDocumento64 páginasPresented by DR Rahul D AgrawalRahul AgrawalAinda não há avaliações
- Robbins Basic Pathology 9th Edition Kumar Test BankDocumento6 páginasRobbins Basic Pathology 9th Edition Kumar Test Bankvolitiveacrosporedur100% (26)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- Ischemic Heart DiseaseDocumento116 páginasIschemic Heart DiseaseAndrew OrlovAinda não há avaliações
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Topnotch ECG Interpretation For MoonlightersDocumento25 páginasTopnotch ECG Interpretation For Moonlightersmefav7778520100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
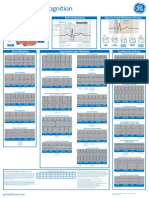
- Arrhythmia Recognition Part 1 and 2 DOC1178264 Rev2Documento2 páginasArrhythmia Recognition Part 1 and 2 DOC1178264 Rev2Nico Angelo CopoAinda não há avaliações
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- Clinical Implications of Left Atrial Enlargement - A ReviewDocumento6 páginasClinical Implications of Left Atrial Enlargement - A ReviewRMO RSJDAinda não há avaliações
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Prognosis and Outcomes Following Sudden Cardiac Arrest in AdultsDocumento24 páginasPrognosis and Outcomes Following Sudden Cardiac Arrest in AdultsAnca StanAinda não há avaliações
- ACLSDocumento61 páginasACLSmgthida935100% (1)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Coronary Artery DiseaseDocumento33 páginasCoronary Artery DiseaseAlma Rifa'Ana LiskaAinda não há avaliações
- Pha CPR Bls Acls Manual 2012 Edited (08 25 2012)Documento30 páginasPha CPR Bls Acls Manual 2012 Edited (08 25 2012)Gene Alfonso BanawaAinda não há avaliações
- I. Skenario A: 2. Muffle Heart SoundsDocumento6 páginasI. Skenario A: 2. Muffle Heart SoundsJefri SoniAinda não há avaliações
- Antiarrhythmic Drugs: AmiodaroneDocumento32 páginasAntiarrhythmic Drugs: Amiodaroneabd hamzaAinda não há avaliações
- Cardiac Rhythms - ECG ReadingsDocumento15 páginasCardiac Rhythms - ECG Readingsal-obinay shereenAinda não há avaliações
- Chap22 PDFDocumento9 páginasChap22 PDFSam CryshnaAinda não há avaliações
- Adams-Stokes 1º Sintoma Febre ReumáticaDocumento5 páginasAdams-Stokes 1º Sintoma Febre Reumáticacarvalho.tr4270Ainda não há avaliações
- 20 Questions HypothermiaDocumento8 páginas20 Questions HypothermiaManuelAinda não há avaliações
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- DefibrillationDocumento11 páginasDefibrillationarchumeenabaluAinda não há avaliações
- 1500 Ebook Clinical Medicine Up PDFDocumento215 páginas1500 Ebook Clinical Medicine Up PDFAhmad Arif100% (1)
- ACLS and MegacodeDocumento33 páginasACLS and MegacodeMark Joseph100% (1)
- Erc - 2005Documento58 páginasErc - 2005zulfantri1983Ainda não há avaliações
- Crash Cart Lecture-WhiteDocumento103 páginasCrash Cart Lecture-WhiteMarianne Laylo67% (3)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- List of Empanelled HCOs-Jaipur As On 20 December 2022Documento24 páginasList of Empanelled HCOs-Jaipur As On 20 December 2022SATYAJIT PALAinda não há avaliações