Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
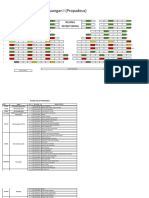
- Case 2 - Breakeven Analysis PDFDocumento3 páginasCase 2 - Breakeven Analysis PDFAnnie Anna0% (1)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Autorizacion CirugiaDocumento1 páginaAutorizacion Cirugiaanon_375322244Ainda não há avaliações
- Saint Alphonsus Statement On LettersDocumento1 páginaSaint Alphonsus Statement On LettersKBOI 2NewsAinda não há avaliações
- Jupiter EngDocumento34 páginasJupiter EngakukauakuAinda não há avaliações
- HAP & VAP IDSA Pocketcard Guidelines (2016)Documento12 páginasHAP & VAP IDSA Pocketcard Guidelines (2016)David GerickAinda não há avaliações
- Adultand Adolescent GLDocumento460 páginasAdultand Adolescent GLMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- Diabetic Foot Infection: A challenge for primary and secondary careDocumento35 páginasDiabetic Foot Infection: A challenge for primary and secondary careMuhammad DaviqAinda não há avaliações
- Prevalence of Hypoalbuminemia in Outpatients With HIV/AIDS: ArticleDocumento5 páginasPrevalence of Hypoalbuminemia in Outpatients With HIV/AIDS: ArticleMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- Adult OIDocumento509 páginasAdult OIMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- 18c. Lymphoma EditedDocumento36 páginas18c. Lymphoma EditedMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- 18c. Lymphoma 1editedDocumento36 páginas18c. Lymphoma 1editedMuhammad DaviqAinda não há avaliações
- 11c. Tambahan Saja RTD Gresik 2 FinalDocumento76 páginas11c. Tambahan Saja RTD Gresik 2 FinalMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- 21b. Hipertiroid FKDocumento15 páginas21b. Hipertiroid FKMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- UJian PPDsDocumento9 páginasUJian PPDsMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- 17b. Myelodysplastic Syndrome Rev 2016Documento15 páginas17b. Myelodysplastic Syndrome Rev 2016MUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- Sony Wicaksono Susanto Nugroho: Lab/SMF Ilmu Kesehatan Anak FK Universitas Brawijaya/RS Dr. Saiful AnwarDocumento39 páginasSony Wicaksono Susanto Nugroho: Lab/SMF Ilmu Kesehatan Anak FK Universitas Brawijaya/RS Dr. Saiful AnwarMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- Dr. Handoko T, SPP: Sub Departemen Penyakit Paru Dan AlergiDocumento54 páginasDr. Handoko T, SPP: Sub Departemen Penyakit Paru Dan AlergiMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- Rheumatology (4) 2015Documento59 páginasRheumatology (4) 2015MUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- 9a. Red Cell DisordersDocumento46 páginas9a. Red Cell DisordersMuhammad DaviqAinda não há avaliações
- Acute Lung Edema (Pulmo)Documento35 páginasAcute Lung Edema (Pulmo)Muhammad DaviqAinda não há avaliações
- Doctoring 3, Diabetes MellitusDocumento62 páginasDoctoring 3, Diabetes MellitusMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- 2d) Patofisiologi Sesak Napas by Dr. AminuddinDocumento39 páginas2d) Patofisiologi Sesak Napas by Dr. AminuddinMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- Understanding Bleeding Disorders: Pathogenesis and Pathophysiology of ITP, Hemophilia, and VKDBDocumento45 páginasUnderstanding Bleeding Disorders: Pathogenesis and Pathophysiology of ITP, Hemophilia, and VKDBMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- Ost ArthritisDocumento38 páginasOst Arthritismega_ayuAinda não há avaliações
- Hyperglycemic Hyperosmolar Syndrome: Sidarti Soehita SFHS Dept - of Clinical Pathology Airlangga University Medical FacultyDocumento7 páginasHyperglycemic Hyperosmolar Syndrome: Sidarti Soehita SFHS Dept - of Clinical Pathology Airlangga University Medical FacultyMuhammad DaviqAinda não há avaliações
- Tes Rivalta (Transudat-Eksudat)Documento13 páginasTes Rivalta (Transudat-Eksudat)Sulyasti nomleni0% (1)
- Dokter Dan Sarjana PDFDocumento4.411 páginasDokter Dan Sarjana PDFmomonomomAinda não há avaliações
- 2d) Patofisiologi Sesak Napas by Dr. AminuddinDocumento39 páginas2d) Patofisiologi Sesak Napas by Dr. AminuddinMUHAMMAD BAGIR ALJUFRIAinda não há avaliações
- Current Trends in PharmacovigilanceDocumento5 páginasCurrent Trends in PharmacovigilanceSutirtho MukherjiAinda não há avaliações
- Aiswarya Krishna: Professional SummaryDocumento4 páginasAiswarya Krishna: Professional SummaryRejoy RadhakrishnanAinda não há avaliações
- LeprosyDocumento9 páginasLeprosyJohn Ribu Parampil100% (1)
- Morning Report September, 10 2015: Supervisor: Dr. Agus Thoriq, Spog DM Jaga: RianDocumento15 páginasMorning Report September, 10 2015: Supervisor: Dr. Agus Thoriq, Spog DM Jaga: RianRian Segal HidajatAinda não há avaliações
- Lab Technician or Clerical or BankingDocumento2 páginasLab Technician or Clerical or Bankingapi-76931734Ainda não há avaliações
- October 2017 Ophthalmic PearlsDocumento3 páginasOctober 2017 Ophthalmic PearlsShafa KhansaAinda não há avaliações
- November 8, 2014Documento16 páginasNovember 8, 2014The Delphos HeraldAinda não há avaliações
- Bumrungrad HospitalDocumento3 páginasBumrungrad HospitalAhmadnur kholilAinda não há avaliações
- Tracheo-Oesophageal FistulaDocumento19 páginasTracheo-Oesophageal Fistularajan kumar100% (3)
- LOG BOOK For Objective Assessment C-P I & II KMUDocumento13 páginasLOG BOOK For Objective Assessment C-P I & II KMUFarhaanKhanHaleem100% (3)
- The Crusades and Ancient Medical TheoryDocumento3 páginasThe Crusades and Ancient Medical TheoryJordan Tyler VoltzAinda não há avaliações
- Assessing Body TemperatureDocumento6 páginasAssessing Body TemperatureemailAinda não há avaliações
- 52 - CBD OilDocumento29 páginas52 - CBD OilMarijo Duišin100% (6)
- Assessment of MalingeringDocumento12 páginasAssessment of MalingeringkosmicAinda não há avaliações
- Close Fracture Radius Ulna Distal Sinistra: Case ReportDocumento30 páginasClose Fracture Radius Ulna Distal Sinistra: Case ReportyoyokAinda não há avaliações
- Drug Development: FDA's Definition of A New DrugDocumento11 páginasDrug Development: FDA's Definition of A New DrugSophie MendezAinda não há avaliações
- Antimicrobial ChemotherapyDocumento160 páginasAntimicrobial Chemotherapyokumu atanas0% (1)
- Eeg BookDocumento102 páginasEeg BookmacrufoAinda não há avaliações
- Survival Strategies For Parenting The Child & Teen With BipolarDocumento236 páginasSurvival Strategies For Parenting The Child & Teen With Bipolarseptiadhi wirawanAinda não há avaliações
- Geriatri 1Documento6 páginasGeriatri 1KemasNugrohoAinda não há avaliações
- Ross Case Book 2016Documento305 páginasRoss Case Book 2016S86% (7)
- CRAFFTDocumento24 páginasCRAFFTRani HusainAinda não há avaliações
- Article - Quick REMAP - Steps in The Quick REMAP4-point Rapid Relief Protocol 1 PDFDocumento32 páginasArticle - Quick REMAP - Steps in The Quick REMAP4-point Rapid Relief Protocol 1 PDFAnonymous g8zT2sPtjW100% (1)
- Janie Jacobs Resume March 2019Documento2 páginasJanie Jacobs Resume March 2019api-404179099Ainda não há avaliações
- Vaginal Yeast InfectionsDocumento7 páginasVaginal Yeast InfectionsAnimesh PriyaAinda não há avaliações