Você também pode gostar
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Atrial FibrilationDocumento27 páginasAtrial FibrilationemialevelaAinda não há avaliações
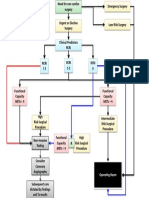
- CIED Surgical Guidance Dec21Documento16 páginasCIED Surgical Guidance Dec21SamAinda não há avaliações
- Transport System in Plants and AnimalsDocumento7 páginasTransport System in Plants and AnimalsBeatriz gannabanAinda não há avaliações
- 3 Statins (Atorvastatin & Rosuvastatin)Documento15 páginas3 Statins (Atorvastatin & Rosuvastatin)Thet Su LwinAinda não há avaliações
- Medication - ALT-Template - AmlodipineDocumento1 páginaMedication - ALT-Template - AmlodipineNancyAmissahAinda não há avaliações
- Appropriation Weeks 4-5Documento6 páginasAppropriation Weeks 4-5AURA CAMILA LEÓN ÁLVAREZAinda não há avaliações
- Infant CPRDocumento1 páginaInfant CPRDaniica MacaranasAinda não há avaliações
- Ward ClassDocumento1 páginaWard ClassJulius Elfred ValenzonaAinda não há avaliações
- Basic ECG Analysis and Interpretation SkillsDocumento46 páginasBasic ECG Analysis and Interpretation SkillsSumeet TripathiAinda não há avaliações
- HypertensionDocumento2 páginasHypertensionRodel Yacas0% (1)
- Journal of Cardiology + RomanaDocumento120 páginasJournal of Cardiology + RomanaMiss Oana100% (1)
- Cover Letter For EportfolioDocumento1 páginaCover Letter For Eportfolioapi-302255572Ainda não há avaliações
- Philips Heartstart MRX Defibrillator ManualDocumento383 páginasPhilips Heartstart MRX Defibrillator Manualjose rojasAinda não há avaliações
- Vitalsigns PDFDocumento36 páginasVitalsigns PDFSuneel Kumar PrajapatiAinda não há avaliações
- Aortic DissectionDocumento24 páginasAortic Dissectionsameeha semiAinda não há avaliações
- Jurnal Media Keperawatan: Politeknik Kesehatan Makassar Vol. 11 No. 01 2020 E-Issn: 2087-0035Documento6 páginasJurnal Media Keperawatan: Politeknik Kesehatan Makassar Vol. 11 No. 01 2020 E-Issn: 2087-0035ちかお 千春Ainda não há avaliações
- Essential Nursing Procedures Assignment - 092039Documento14 páginasEssential Nursing Procedures Assignment - 092039IRA MONIQUE CABADENAinda não há avaliações
- Heart Lung InteractionDocumento29 páginasHeart Lung InteractionKARDIOLOGI STASE RSALAinda não há avaliações
- Wasserman 1964Documento9 páginasWasserman 1964jesusleon.lmAinda não há avaliações
- Dabl Educational TrustMonitors For Self-Measurement of Blood Pressure (SBPM)Documento1 páginaDabl Educational TrustMonitors For Self-Measurement of Blood Pressure (SBPM)iranbengoaAinda não há avaliações
- Cardiac Risk Assessemnt FlowchartDocumento1 páginaCardiac Risk Assessemnt FlowchartjamesomooreAinda não há avaliações
- Association of Treatment With Metformin Vs SulfonylureaDocumento11 páginasAssociation of Treatment With Metformin Vs SulfonylureamiguelalmenarezAinda não há avaliações
- Advanced Cardiac Life Support (ACLS)Documento17 páginasAdvanced Cardiac Life Support (ACLS)Siti Rahima HarahapAinda não há avaliações
- Self-Learning Module For Grade 11: Earth and Life Science How Animals Survive How Will You Use This Module?Documento8 páginasSelf-Learning Module For Grade 11: Earth and Life Science How Animals Survive How Will You Use This Module?MIMOYOUAinda não há avaliações
- 10 1161@hypertensionaha 119 14240 PDFDocumento8 páginas10 1161@hypertensionaha 119 14240 PDFAbidia KamilAinda não há avaliações
- Adapta SeriesDocumento354 páginasAdapta SeriesGabriel Pascual ArencibiaAinda não há avaliações
- Common Emergency DrugsDocumento58 páginasCommon Emergency Drugshatem alsrour84% (19)
- 2022 ESC VASCD Guidelines Official Slide Set - Final - ProtectedDocumento23 páginas2022 ESC VASCD Guidelines Official Slide Set - Final - Protectedshamaamo19Ainda não há avaliações
- Test Case 3 H&P - RedactedDocumento9 páginasTest Case 3 H&P - RedactedFernando Galera Jr.Ainda não há avaliações
- Unstable Angina - Cardiovascular Disorders - MSD Manual Professional EditionDocumento1 páginaUnstable Angina - Cardiovascular Disorders - MSD Manual Professional EditionboynextdoorpkyAinda não há avaliações