Você também pode gostar
- Primary Hip Arthroplasty Templating On Standard Radiographs PDFDocumento11 páginasPrimary Hip Arthroplasty Templating On Standard Radiographs PDFmihai popescuAinda não há avaliações
- A Review On Total Hip Replacement: April 2016Documento55 páginasA Review On Total Hip Replacement: April 2016uzlifatil jannahAinda não há avaliações
- Model Release: 2257 Compliance FormDocumento4 páginasModel Release: 2257 Compliance FormmarkhuzAinda não há avaliações
- Fitmore Hip Surgical TechniqueDocumento24 páginasFitmore Hip Surgical TechniqueAdrian TudorAinda não há avaliações
- DPEM ORT 0812 0182a 1 - LRDocumento32 páginasDPEM ORT 0812 0182a 1 - LRVladimir NikopolAinda não há avaliações
- Sink or Shine: Attract Clients and Talent With the Brightness of Your MissionNo EverandSink or Shine: Attract Clients and Talent With the Brightness of Your MissionAinda não há avaliações
- 2015FMetallic Implant BiomaterialsDocumento57 páginas2015FMetallic Implant BiomaterialsAlicia Jara ChavezAinda não há avaliações
- Types of BacklinksDocumento1 páginaTypes of BacklinksBad BoyAinda não há avaliações
- BACKLINKSDocumento1 páginaBACKLINKSSoumil KuraniAinda não há avaliações
- Artificial Hip Joint/Hip Replacement: Muhammad Akmal Qaisar 08-PWMCT-0056 Mechanical Engg DesignDocumento18 páginasArtificial Hip Joint/Hip Replacement: Muhammad Akmal Qaisar 08-PWMCT-0056 Mechanical Engg DesignAkmalAinda não há avaliações
- Aspects of Orthopedic Implants and Prostheses Materials. Processing Technologies.Documento6 páginasAspects of Orthopedic Implants and Prostheses Materials. Processing Technologies.Nurul AsyilahAinda não há avaliações
- Eduonix Digital MarketingDocumento17 páginasEduonix Digital MarketingEduonix JavascriptAinda não há avaliações
- Brand Equity HPDocumento32 páginasBrand Equity HPgakare_rakeshAinda não há avaliações
- OTT Media MonetizationDocumento25 páginasOTT Media MonetizationSubish PunnooseAinda não há avaliações
- Buyer Persona TemplateDocumento19 páginasBuyer Persona TemplateCitra resmiAinda não há avaliações
- Strategic Management Individual Assignment: Critique On Disney Goes OTT: The Launch That Defined A Major Industry ShiftDocumento8 páginasStrategic Management Individual Assignment: Critique On Disney Goes OTT: The Launch That Defined A Major Industry ShiftShivam TiwariAinda não há avaliações
- Brand Equity ModelsDocumento20 páginasBrand Equity ModelsVarunSinghAinda não há avaliações
- b2b PPT FinalDocumento26 páginasb2b PPT FinalRaj Kothari MAinda não há avaliações
- Biomedical Engineering MinicourseDocumento54 páginasBiomedical Engineering MinicourseDaniela Tanase100% (1)
- How To Create An Email Id and Send EmailDocumento16 páginasHow To Create An Email Id and Send EmailpreetgodanAinda não há avaliações
- Opinion Mining On Social Media Data: 2013 IEEE 14th International Conference On Mobile Data ManagementDocumento6 páginasOpinion Mining On Social Media Data: 2013 IEEE 14th International Conference On Mobile Data ManagementsenthilnathanAinda não há avaliações
- Youtube For BrandsDocumento33 páginasYoutube For BrandsAomlet TanatonAinda não há avaliações
- Adwords Formula CalculatorDocumento1 páginaAdwords Formula CalculatorAlan CristianAinda não há avaliações
- Afaqs Reporter CompressedDocumento80 páginasAfaqs Reporter CompressedPankaj VinayakAinda não há avaliações
- Development of Tourism in Dubai Grace Chang MazzaDocumento24 páginasDevelopment of Tourism in Dubai Grace Chang MazzaMohit AroraAinda não há avaliações
- Customer Relationship Marketing - MarketingDocumento14 páginasCustomer Relationship Marketing - Marketingtiffani_88103892Ainda não há avaliações
- Google AnalyticsDocumento13 páginasGoogle AnalyticsPaul S100% (1)
- Wembley StadiumDocumento2 páginasWembley StadiumVanessaAinda não há avaliações
- SEO Onpage TemplateDocumento39 páginasSEO Onpage TemplateUmair HashmiAinda não há avaliações
- 3036 BriefDocumento2 páginas3036 BriefNaufalMuhammadSiddiqAinda não há avaliações
- Brand Equity Measurement: HappydentDocumento26 páginasBrand Equity Measurement: Happydentgm.kayal0% (1)
- Pre Operative Planning For Total Hip ArthroplastyDocumento78 páginasPre Operative Planning For Total Hip ArthroplastyJulio EspinozaAinda não há avaliações
- TechniqueDocumento7 páginasTechniqueFlorin MacarieAinda não há avaliações
- Step by Step Guide How To Template The Hip: Lustig Sébastien MD, PHD, Prof Albert Trillat Center - Lyon - FranceDocumento25 páginasStep by Step Guide How To Template The Hip: Lustig Sébastien MD, PHD, Prof Albert Trillat Center - Lyon - FranceAlaa ElbulukAinda não há avaliações
- 10 FractureFixationOsteoporotic FINAL 10913Documento77 páginas10 FractureFixationOsteoporotic FINAL 10913Pankaj VatsaAinda não há avaliações
- Upload Scribd 3Documento5 páginasUpload Scribd 3Yoga AninditaAinda não há avaliações
- UCLA Upper Extremity Amputations Manual - Sholder ProsthesisDocumento39 páginasUCLA Upper Extremity Amputations Manual - Sholder ProsthesisAlaa SalamAinda não há avaliações
- High Hip Center in Total Hip Arthroplasty With Acetabular DeficiencyDocumento21 páginasHigh Hip Center in Total Hip Arthroplasty With Acetabular DeficiencyIvana LmsAinda não há avaliações
- Positioning Techniques For Lower ExtremitiesDocumento80 páginasPositioning Techniques For Lower ExtremitiesChu emmanuel ndzeAinda não há avaliações
- Surgical Approaches of Dorsal SpineDocumento36 páginasSurgical Approaches of Dorsal SpineWaqas Saeed BaqaiAinda não há avaliações
- Corail Surgical Technique Revision 1Documento20 páginasCorail Surgical Technique Revision 1Kaustubh KeskarAinda não há avaliações
- Carpal InstabilityDocumento83 páginasCarpal Instabilityshammasbm100% (1)
- Hinge Axis and FacebowDocumento80 páginasHinge Axis and FacebowDrSadaf KazmiAinda não há avaliações
- Alingment in TKRDocumento3 páginasAlingment in TKRdeepak100% (1)
- NexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29Documento48 páginasNexGen Flexion Balancing Instruments Surgical Technique 2897-5967-031-00 Rev1!29!2811 2009 29flo1987Ainda não há avaliações
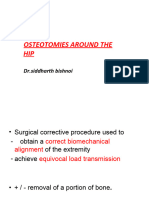
- Osteotomiesaroundthehip 160203173448Documento130 páginasOsteotomiesaroundthehip 160203173448Mit ParikhAinda não há avaliações
- Surgical Technique For Combined D Wyer Calcaneal Osteotomy and PeronealDocumento6 páginasSurgical Technique For Combined D Wyer Calcaneal Osteotomy and PeronealleahbayAinda não há avaliações
- Levels of AmputationsDocumento6 páginasLevels of AmputationsJuanitoCabatañaLimIII100% (1)
- CorailDocumento18 páginasCorailXeniaAinda não há avaliações
- 1-Prof DR Anees Biomechanics of HipDocumento63 páginas1-Prof DR Anees Biomechanics of HipAhmed M3tmdAinda não há avaliações
- Anterolateral Approach of Proximal Humerus + Henry ApproachDocumento33 páginasAnterolateral Approach of Proximal Humerus + Henry ApproachwildanmalikAinda não há avaliações
- Natural History of AISDocumento42 páginasNatural History of AISJosh JoshiAinda não há avaliações
- Facebow Calliper ReviewDocumento5 páginasFacebow Calliper ReviewFaheemuddin Muhammad100% (3)
- TracingDocumento9 páginasTracingBharath KondaveetiAinda não há avaliações
- Anterior Cervical VertebrectomyDocumento4 páginasAnterior Cervical VertebrectomyGabriela MacoveanuAinda não há avaliações
- U2 Knee Ps TecnicaDocumento52 páginasU2 Knee Ps TecnicaIsabella MarulandaAinda não há avaliações
- A AaaaaaaDocumento6 páginasA AaaaaaaAnonymous d9Bzr1Ainda não há avaliações
- Journal of Orthopaedic Surgery and ResearchDocumento6 páginasJournal of Orthopaedic Surgery and ResearchDewye SartikaAinda não há avaliações
- Orthodontics: Cephalometric Analysis Cephalometric Landmarks, Planes & AnglesDocumento11 páginasOrthodontics: Cephalometric Analysis Cephalometric Landmarks, Planes & AnglesQueen LiveAinda não há avaliações
- Jurnal 5Documento7 páginasJurnal 5JAQUELINEAinda não há avaliações
- Hip Fractures Current Review of TreatmentDocumento1 páginaHip Fractures Current Review of TreatmentMarius ChirilaAinda não há avaliações
- Acute Scapholunate and Lunotriquetral Dissociation PDFDocumento19 páginasAcute Scapholunate and Lunotriquetral Dissociation PDFMarius ChirilaAinda não há avaliações
- Stabilization of Acute High-Grade Acromioclavicular Joint SeparationDocumento10 páginasStabilization of Acute High-Grade Acromioclavicular Joint SeparationMarius ChirilaAinda não há avaliações
- March, 13-14: International SymposiumDocumento9 páginasMarch, 13-14: International SymposiumMarius ChirilaAinda não há avaliações
- Englert2013 PDFDocumento12 páginasEnglert2013 PDFMarius ChirilaAinda não há avaliações
- Cable Ready Cable Grip System Cable Buttons Surgical Technique PDFDocumento2 páginasCable Ready Cable Grip System Cable Buttons Surgical Technique PDFMarius ChirilaAinda não há avaliações
- Apricot SurgicalTechniqueDocumento13 páginasApricot SurgicalTechniqueMarius ChirilaAinda não há avaliações
- 112-1 中英筆譯Documento15 páginas112-1 中英筆譯beenbenny825Ainda não há avaliações
- The Law of Attraction Work For YouDocumento7 páginasThe Law of Attraction Work For YouBambang PrasetyoAinda não há avaliações
- Principal Parts of Greek Verbs Appearing in James SwetnamDocumento8 páginasPrincipal Parts of Greek Verbs Appearing in James Swetnammausj100% (1)
- Breast Stimulation Susilowati 2004138Documento11 páginasBreast Stimulation Susilowati 2004138Ahmad SaifuddinAinda não há avaliações
- Case MyelitisDocumento34 páginasCase Myelitisyolanda nurlizaAinda não há avaliações
- Daily Lesson LogDocumento6 páginasDaily Lesson LogNicoleMortelAinda não há avaliações
- Journal of The Neurological Sciences: SciencedirectDocumento12 páginasJournal of The Neurological Sciences: SciencedirectBotez MartaAinda não há avaliações
- Readable Elaine Kirn - Pamela Hartmenn, - 2009 - Interactions 1 - EnG 106 - 2020S - TEXTDocumento256 páginasReadable Elaine Kirn - Pamela Hartmenn, - 2009 - Interactions 1 - EnG 106 - 2020S - TEXTle huy100% (1)
- How Emotionally Intelligent Are You Wong and Law Emotional Intelligence Scale WLEISDocumento2 páginasHow Emotionally Intelligent Are You Wong and Law Emotional Intelligence Scale WLEISIsabela Bică100% (2)
- Ir21 Geomt 2022-01-28Documento23 páginasIr21 Geomt 2022-01-28Master MasterAinda não há avaliações
- Deluxe SolutionDocumento6 páginasDeluxe SolutionR K Patham100% (1)
- Calle Zorro - Penis Size ParanoiaDocumento0 páginaCalle Zorro - Penis Size ParanoiaAquarius Sharp BladeAinda não há avaliações
- Rectification of Errors - QuestionsDocumento6 páginasRectification of Errors - QuestionsBhargav RavalAinda não há avaliações
- Hernia Examination OSCE Guide PDFDocumento8 páginasHernia Examination OSCE Guide PDFParsaant SinghAinda não há avaliações
- Reading Comprehension TextsDocumento15 páginasReading Comprehension TextsCMRotaruAinda não há avaliações
- Answers For TimesetDocumento11 páginasAnswers For TimesetMuntazirAinda não há avaliações
- Rayya Abdallah David Abdallah, As Next of Kin of Baby Boy Abdallah, and On Their Own Personal Behalf v. Wilbur Callender, M.D. Government of The Virgin Islands, 1 F.3d 141, 3rd Cir. (1993)Documento13 páginasRayya Abdallah David Abdallah, As Next of Kin of Baby Boy Abdallah, and On Their Own Personal Behalf v. Wilbur Callender, M.D. Government of The Virgin Islands, 1 F.3d 141, 3rd Cir. (1993)Scribd Government DocsAinda não há avaliações
- USA v. William Gazafi Plea Letter To Judge TitusDocumento13 páginasUSA v. William Gazafi Plea Letter To Judge TitusSouthern Maryland OnlineAinda não há avaliações
- (JPN) - E-Hand Book UpdatedDocumento31 páginas(JPN) - E-Hand Book UpdatedjainvaibhiAinda não há avaliações
- The Best WayDocumento58 páginasThe Best Wayshiela manalaysayAinda não há avaliações
- 2 Cor 37Documento2 páginas2 Cor 37M. Div ChoudhrayAinda não há avaliações
- 11 Rabino v. Cruz 222 SCRA 493Documento4 páginas11 Rabino v. Cruz 222 SCRA 493Joshua Janine LugtuAinda não há avaliações
- Journal of Cognitive Liberties׃ Vol. 4, No. 2 (2003)Documento97 páginasJournal of Cognitive Liberties׃ Vol. 4, No. 2 (2003)HoorayFrisbeeHeadAinda não há avaliações
- Oracle Database Performance Tuning Advanced Features and Best Practices For DbasDocumento303 páginasOracle Database Performance Tuning Advanced Features and Best Practices For Dbassss pppAinda não há avaliações
- Omer Farooq ResumeDocumento3 páginasOmer Farooq ResumemykdesignerAinda não há avaliações
- Contents:: 1. Introduction To Neural NetworksDocumento27 páginasContents:: 1. Introduction To Neural NetworksKarthik VanamAinda não há avaliações
- Report Why EvolveDocumento11 páginasReport Why EvolveMirela OlarescuAinda não há avaliações
- Concept PaperDocumento3 páginasConcept PaperDan Reynald Domingo SomeraAinda não há avaliações
- BM AssignmentDocumento7 páginasBM AssignmentAntony LawrenceAinda não há avaliações
- The Balance of Power in World Politics TDocumento23 páginasThe Balance of Power in World Politics TVali IgnatAinda não há avaliações