Você também pode gostar
- Management of Tuberculosis: A guide for clinicians (eBook edition)No EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Ainda não há avaliações
- 1) BiopsyDocumento30 páginas1) BiopsySosa GeorgeAinda não há avaliações
- Riaz Gul AHN Unit 1Documento106 páginasRiaz Gul AHN Unit 1Riaz Gul RindAinda não há avaliações
- Seminar On MastectomyDocumento8 páginasSeminar On Mastectomypooja singhAinda não há avaliações
- Shock Concept MapDocumento2 páginasShock Concept MapElizabeth GarretsonAinda não há avaliações
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Muscle Strength TestingDocumento3 páginasMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- Skin Cancer!Documento8 páginasSkin Cancer!HudiansyahAinda não há avaliações
- Urinary CatheterizationDocumento2 páginasUrinary CatheterizationFains YdbwidAinda não há avaliações
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Warning Signs of Various DiseasesDocumento44 páginasWarning Signs of Various DiseasesamsabavanAinda não há avaliações
- HYDROCEPHALUSDocumento63 páginasHYDROCEPHALUSAjeng Aristiany Rahawarin100% (2)
- Ostomy TrainingDocumento37 páginasOstomy Trainingsophia hasanah100% (1)
- Breast CancerDocumento8 páginasBreast CancerJeyser T. Gamutia100% (1)
- Barrier NursingDocumento2 páginasBarrier NursingDrPreeti Thakur ChouhanAinda não há avaliações
- Eye ExaminationDocumento23 páginasEye Examinationcynthia167Ainda não há avaliações
- Intertrigo, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandIntertrigo, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Cytotoxic ChemotherapyDocumento33 páginasCytotoxic ChemotherapyDoniTrinandaAinda não há avaliações
- Perioperative Nursing Theory ClassDocumento10 páginasPerioperative Nursing Theory Classtwinklesheila3182Ainda não há avaliações
- Nursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalDocumento55 páginasNursing Care of Patients Receiving Chemotherapy Ranjita Rajesh Lecturer People's College of Nursing BhopalFayizatul AkmarAinda não há avaliações
- How Does Radiation Therapy Work?Documento5 páginasHow Does Radiation Therapy Work?mikeadrianAinda não há avaliações
- Zollinger Ellis Wps OfficeDocumento15 páginasZollinger Ellis Wps OfficeAbhash MishraAinda não há avaliações
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsAinda não há avaliações
- Draping The Operative ClientDocumento7 páginasDraping The Operative ClientZIAN LABADIAAinda não há avaliações
- Cervical Cancer ScreeningDocumento25 páginasCervical Cancer Screening6ixSideCreate MAinda não há avaliações
- Insisi Bedah 22 PDFDocumento36 páginasInsisi Bedah 22 PDFMiftah AjiAinda não há avaliações
- Gas GangreneDocumento6 páginasGas GangreneIwan AchmadiAinda não há avaliações
- Maxillary Sinus CarcinomaDocumento4 páginasMaxillary Sinus CarcinomaSuresh MettaAinda não há avaliações
- BIOPSYDocumento8 páginasBIOPSYASHLEY DAWN BUENAFEAinda não há avaliações
- Injection TechniquesDocumento11 páginasInjection TechniquesLeon OngAinda não há avaliações
- Disorders of The Eye OriginalDocumento115 páginasDisorders of The Eye OriginalKwabena AmankwaAinda não há avaliações
- Preoperative Skin PreparationDocumento16 páginasPreoperative Skin PreparationSyahri DzikriAinda não há avaliações
- WK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TideDocumento43 páginasWK13 CDN - Meningitis, Poliomyelitis, Leprosy, Tetanus, Red TidePotato PceeAinda não há avaliações
- CMTC Guj EngDocumento43 páginasCMTC Guj EngSaumilAinda não há avaliações
- Presentation1 Cervical BiopsyDocumento14 páginasPresentation1 Cervical BiopsyChanta MaharjanAinda não há avaliações
- Lesions PPT NewDocumento37 páginasLesions PPT NewDeb SharmaAinda não há avaliações
- Name: Rustia, Nina Dianne R. Year and Section: Level 2-B Subject: RLE: OPD (Reporting) Suture RemovalDocumento4 páginasName: Rustia, Nina Dianne R. Year and Section: Level 2-B Subject: RLE: OPD (Reporting) Suture RemovalNiña Dianne Rubin RustiaAinda não há avaliações
- Skin Premalignant and TumorsDocumento95 páginasSkin Premalignant and TumorsmedicoprakashAinda não há avaliações
- DR - Monobina Sarker (Moic, Ccu) : Howrah District HospitalDocumento56 páginasDR - Monobina Sarker (Moic, Ccu) : Howrah District HospitalDeepa BhattacharjeeAinda não há avaliações
- Choriocarcinoma 11Documento23 páginasChoriocarcinoma 11Fakhir HasanAinda não há avaliações
- Trichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCDocumento27 páginasTrichiasis: Prepared By:pooja Adhikari Roll No.: 27 SMTCsushma shresthaAinda não há avaliações
- Oncology-Study of Cancer Cellular AbberationDocumento43 páginasOncology-Study of Cancer Cellular AbberationIrwan M. IskoberAinda não há avaliações
- Port A CathDocumento14 páginasPort A CathMerika JimenezAinda não há avaliações
- Bone Marrow Aspiration and BiopsyDocumento2 páginasBone Marrow Aspiration and Biopsyprince10120% (1)
- Immediate Newborn Care. BlanksDocumento11 páginasImmediate Newborn Care. BlanksMay Princes Torregosa Abucejo100% (1)
- PericarditisDocumento14 páginasPericarditisinterna MANADOAinda não há avaliações
- Ostomy CareDocumento3 páginasOstomy CareSyamsul ArifinAinda não há avaliações
- Ophthalmia NeonatorumDocumento19 páginasOphthalmia NeonatorumJisha Annie JohnAinda não há avaliações
- Bites and Stings PPT Fix DR IsyaDocumento61 páginasBites and Stings PPT Fix DR IsyamadeAinda não há avaliações
- Cerebral AngiographyDocumento9 páginasCerebral AngiographyVincent LopezAinda não há avaliações
- Postoperative Nursing CareDocumento2 páginasPostoperative Nursing CareYeana AlonAinda não há avaliações
- SinusitisDocumento37 páginasSinusitismalathiAinda não há avaliações
- Cardiac TestsDocumento17 páginasCardiac TestsGiorgiana pAinda não há avaliações
- Breast CancerDocumento52 páginasBreast CancerLorelie AsisAinda não há avaliações
- Epidemiology, Pathology, Clinical Features, and Diagnosis of Meningioma - UpToDateDocumento22 páginasEpidemiology, Pathology, Clinical Features, and Diagnosis of Meningioma - UpToDatewilson kores100% (1)
- Thoracentesis Is Also Known As Pleural Fluid AnalysisDocumento3 páginasThoracentesis Is Also Known As Pleural Fluid AnalysisJ.r. MercadoAinda não há avaliações
- 1-Polo - MSDSDocumento5 páginas1-Polo - MSDSSaad IqbalAinda não há avaliações
- Material Safety Data Sheet: Coated Bleach Board - ElegantDocumento5 páginasMaterial Safety Data Sheet: Coated Bleach Board - ElegantSaad IqbalAinda não há avaliações
- Technical Data Sheet: Century Paper & Board Mills LimitedDocumento1 páginaTechnical Data Sheet: Century Paper & Board Mills LimitedSaad IqbalAinda não há avaliações
- Technical Data Sheet: Century Paper & Board Mills LimitedDocumento1 páginaTechnical Data Sheet: Century Paper & Board Mills LimitedSaad IqbalAinda não há avaliações
- Technical Data Sheet: Century Paper & Board Mills LimitedDocumento1 páginaTechnical Data Sheet: Century Paper & Board Mills LimitedSaad IqbalAinda não há avaliações
- 2 Impressions TdsDocumento1 página2 Impressions TdsSaad IqbalAinda não há avaliações
- Material Safety Data Sheet: Photocopier Paper - ImpressionDocumento5 páginasMaterial Safety Data Sheet: Photocopier Paper - ImpressionSaad IqbalAinda não há avaliações
- 1 Century MsdsDocumento5 páginas1 Century MsdsSaad IqbalAinda não há avaliações
- Technical Data Sheet: Century Paper & Board Mills LimitedDocumento1 páginaTechnical Data Sheet: Century Paper & Board Mills LimitedSaad IqbalAinda não há avaliações
- 1 Captain MsdsDocumento5 páginas1 Captain MsdsSaad IqbalAinda não há avaliações
- Interflow NDA Systech Products 2020Documento3 páginasInterflow NDA Systech Products 2020Saad IqbalAinda não há avaliações
- iIZVxQEWE2TBJOzMVPp6ytEeoHC3Pm7JySatwI5I PDFDocumento6 páginasiIZVxQEWE2TBJOzMVPp6ytEeoHC3Pm7JySatwI5I PDFSaad Iqbal100% (1)
- 1 Royals MsdsDocumento5 páginas1 Royals MsdsSaad IqbalAinda não há avaliações
- iIZVxQEWE2TBJOzMVPp6ytEeoHC3Pm7JySatwI5I PDFDocumento6 páginasiIZVxQEWE2TBJOzMVPp6ytEeoHC3Pm7JySatwI5I PDFSaad Iqbal100% (1)
- SITE Association MembersDocumento30 páginasSITE Association MembersSaad Iqbal83% (6)
- Technical Data Sheet: Century Paper & Board Mills LimitedDocumento1 páginaTechnical Data Sheet: Century Paper & Board Mills LimitedSaad IqbalAinda não há avaliações
- Company Name Plot Sector Representative S.No. Mem. No. Title Cnic #Documento47 páginasCompany Name Plot Sector Representative S.No. Mem. No. Title Cnic #Saad IqbalAinda não há avaliações
- Lcci Exporter 2019Documento318 páginasLcci Exporter 2019Vivek Domadia100% (2)
- List of Industries Located in District Malir L.I.A. (Landhi)Documento28 páginasList of Industries Located in District Malir L.I.A. (Landhi)Saad Iqbal100% (2)
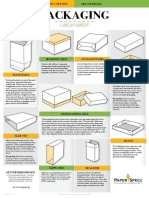
- PaperSpecs PackagingCheatSheetDocumento1 páginaPaperSpecs PackagingCheatSheetSaad IqbalAinda não há avaliações
- Members Data PDFDocumento10 páginasMembers Data PDFSaad IqbalAinda não há avaliações
- Members DataDocumento1.687 páginasMembers DataSAADTECHIE88% (8)
- Akbar Food: View MoreDocumento2 páginasAkbar Food: View MoreSaad IqbalAinda não há avaliações
- Akbar Food: View MoreDocumento2 páginasAkbar Food: View MoreSaad IqbalAinda não há avaliações
- Coso - Monitoring QuestionnaireDocumento1 páginaCoso - Monitoring QuestionnaireSaad IqbalAinda não há avaliações
- Resume: Saad Iqbal / Business Development & OperationsDocumento5 páginasResume: Saad Iqbal / Business Development & OperationsSaad IqbalAinda não há avaliações
- Resume: Saad Iqbal / Business Development & OperationsDocumento5 páginasResume: Saad Iqbal / Business Development & OperationsSaad IqbalAinda não há avaliações
- EVC Isquemico AHADocumento52 páginasEVC Isquemico AHAalejandromagno1984Ainda não há avaliações
- Pediatrics MCQs - DR Ranjan Singh - Part 2Documento10 páginasPediatrics MCQs - DR Ranjan Singh - Part 2k sagarAinda não há avaliações
- Camel AnesthesiaDocumento16 páginasCamel Anesthesiamuhammad zeeshan ansarAinda não há avaliações
- Acetaminophen Poisoning Cases - SeptiDocumento15 páginasAcetaminophen Poisoning Cases - SeptiseptianasptrAinda não há avaliações
- Asking Reporting Health Problems & Diagnosing: OlehDocumento5 páginasAsking Reporting Health Problems & Diagnosing: Olehsindimei alvianiAinda não há avaliações
- Primary HyperparathyroidismDocumento9 páginasPrimary HyperparathyroidismJamesAinda não há avaliações
- Field Health Services Information System: Annual Report 2012Documento511 páginasField Health Services Information System: Annual Report 2012Gina MabansagAinda não há avaliações
- 429 FT0 Physiotherapy in Obstetrics Gynaecology Mohd. JavedDocumento86 páginas429 FT0 Physiotherapy in Obstetrics Gynaecology Mohd. JavedRekha Satheesan100% (1)
- CASE REPORT COMPETITION With Identifying FeaturesDocumento12 páginasCASE REPORT COMPETITION With Identifying FeaturesJoel Cesar AtinadoAinda não há avaliações
- Cronicon: Integrative Case Study Supraspinatus Tendinitis and Physical Therapy ManagementDocumento4 páginasCronicon: Integrative Case Study Supraspinatus Tendinitis and Physical Therapy ManagementAnandhu GAinda não há avaliações
- The Importance of Good PostureDocumento1 páginaThe Importance of Good Postureerica thapaAinda não há avaliações
- GE Healthcare AnestesiaDocumento128 páginasGE Healthcare AnestesiaLuis Alberto Jiménez AcataAinda não há avaliações
- Bllod Transfision ConsentDocumento1 páginaBllod Transfision ConsentumeshbhartiAinda não há avaliações
- Kristjansson 2009Documento14 páginasKristjansson 2009AdosotoAinda não há avaliações
- Lap Ok RSGM Ronal HudaDocumento23 páginasLap Ok RSGM Ronal HudaDwi SastrawanAinda não há avaliações
- Ma. Cricel T. Dela Cruz, RMTDocumento4 páginasMa. Cricel T. Dela Cruz, RMTMa. Cricel T. Dela CruzAinda não há avaliações
- Comparison of Hemorrhoid Sclerotherapy Using Glucose 50% vs. Phenol in Olive OilDocumento4 páginasComparison of Hemorrhoid Sclerotherapy Using Glucose 50% vs. Phenol in Olive OilGabrielEnricoPangarianAinda não há avaliações
- Diabetic Foot Care Center:: One Stop Service For The Management of Diabetic Foot ProblemsDocumento29 páginasDiabetic Foot Care Center:: One Stop Service For The Management of Diabetic Foot ProblemsscribdAinda não há avaliações
- 2021 Batangas Medical Center - Updated Citizens Charter HandbookDocumento447 páginas2021 Batangas Medical Center - Updated Citizens Charter HandbookHarlyn MagsinoAinda não há avaliações
- Auricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical CasesDocumento11 páginasAuricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical Casesyan92120Ainda não há avaliações
- ECTDocumento22 páginasECTRubz Bulquerin0% (1)
- BotoxMedical Patient BrochureDocumento21 páginasBotoxMedical Patient BrochurePatricia Avalos C.Ainda não há avaliações
- Complete DenturesDocumento68 páginasComplete DenturesRaja Rahaizat100% (2)
- CPG Management of Diabetic Foot (2nd Ed)Documento76 páginasCPG Management of Diabetic Foot (2nd Ed)Nokoline Hu100% (1)
- Paragonimus Westermani: Dr.T.V.Rao MDDocumento26 páginasParagonimus Westermani: Dr.T.V.Rao MDtummalapalli venkateswara raoAinda não há avaliações
- Drug StudyDocumento7 páginasDrug Studyanne009Ainda não há avaliações
- Parkinson's DiseaseDocumento11 páginasParkinson's DiseaseZA IDAinda não há avaliações
- Role of Pain Placebo Analgesia: Gordont, Fields FDocumento4 páginasRole of Pain Placebo Analgesia: Gordont, Fields Fmaurina rizkiAinda não há avaliações
- Drug Addiction. HvpeDocumento9 páginasDrug Addiction. HvpeMehak NaggarAinda não há avaliações
- (PEDIA) 2.04 Pediatric Neurologic Exam - Dr. Rivera PDFDocumento15 páginas(PEDIA) 2.04 Pediatric Neurologic Exam - Dr. Rivera PDFJudith Dianne IgnacioAinda não há avaliações