Você também pode gostar
- I-1B. Bacterial Infection 2Documento6 páginasI-1B. Bacterial Infection 2Soad ShedeedAinda não há avaliações
- Vaccine Preventable Communicable DiseasesDocumento7 páginasVaccine Preventable Communicable DiseasesmadmarycashAinda não há avaliações
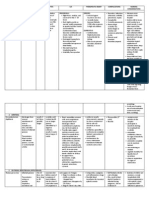
- Synonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsDocumento13 páginasSynonyms Causative Agents Incubatiob Period Mode of Transmission Signs and Symptoms Period of Communicability Diagnostic Test Medical Management Nursing Management ComplicationsYnah DominiqueAinda não há avaliações
- Sexually Transmitted Infections and PregnancyDocumento19 páginasSexually Transmitted Infections and PregnancyBeyins TiuAinda não há avaliações
- Slide - K-21-22 Patogenesis Dan Diagnosis Parasit OportunistikDocumento69 páginasSlide - K-21-22 Patogenesis Dan Diagnosis Parasit OportunistikFaisal AlhasAinda não há avaliações
- Diphtheria HandoutsDocumento8 páginasDiphtheria HandoutsRachelle Mae DimayugaAinda não há avaliações
- Communicable DiseasesDocumento6 páginasCommunicable DiseasesLory LynAinda não há avaliações
- Cdnursing PPT 2021Documento37 páginasCdnursing PPT 2021yuuki konnoAinda não há avaliações
- Eruptive Fever DiseaseDocumento61 páginasEruptive Fever DiseasePearl DiBerardino100% (2)
- Sexually Transmitted DiseaseDocumento3 páginasSexually Transmitted DiseaseBrianna ValerioAinda não há avaliações
- Infectious Disease - BoardsDocumento8 páginasInfectious Disease - BoardsSoojung NamAinda não há avaliações
- Diseases PIDSRDocumento25 páginasDiseases PIDSRaringkinking100% (1)
- Table of Communicable Diseases: Disease Signs & Symptoms Incubation Prevention Chicken PoxDocumento10 páginasTable of Communicable Diseases: Disease Signs & Symptoms Incubation Prevention Chicken PoxKristel_Ramall_6985Ainda não há avaliações
- STDDocumento49 páginasSTDArnzz AgbulosAinda não há avaliações
- In House COMMUNICABLE DISEASES HANDOUTDocumento10 páginasIn House COMMUNICABLE DISEASES HANDOUTniczdelosreyes8Ainda não há avaliações
- Chickenpox & ChlamydialDocumento5 páginasChickenpox & ChlamydialEliezah RodriguezAinda não há avaliações
- Sexually Transmitted DiseasesDocumento120 páginasSexually Transmitted DiseasesGliza Jane100% (4)
- Gonorrhea and SyphilisDocumento55 páginasGonorrhea and Syphilisjoshy221196Ainda não há avaliações
- LimfadenitisDocumento24 páginasLimfadenitisrahmah ningsihAinda não há avaliações
- Neisseria Gonorrhoeae, Sometimes Called The: I. DefinitionDocumento16 páginasNeisseria Gonorrhoeae, Sometimes Called The: I. DefinitionBerle Joy VillanuevaAinda não há avaliações
- Acquired Immunodeficiency SyndromeDocumento33 páginasAcquired Immunodeficiency SyndromeSofia MoniqueAinda não há avaliações
- Acquired Immunodeficiency SyndromeDocumento33 páginasAcquired Immunodeficiency SyndromeSofia MoniqueAinda não há avaliações
- Diphtheria Pertussis TetanusDocumento43 páginasDiphtheria Pertussis TetanusPURVI BARIAAinda não há avaliações
- Infections of The Digestive GlandsDocumento17 páginasInfections of The Digestive GlandsCrystal Lynn Keener SciariniAinda não há avaliações
- HIV InfectionDocumento13 páginasHIV Infectionsun shineAinda não há avaliações
- Mikroorganisme Penyebab Infeksi Pada Sistem Reproduksi2003Documento132 páginasMikroorganisme Penyebab Infeksi Pada Sistem Reproduksi2003anitacharisAinda não há avaliações
- Diptheria Converted 200726175940Documento44 páginasDiptheria Converted 2007261759407dbnf4stjyAinda não há avaliações
- Nursing Care of The Community: Control of Communicable Diseases Instructional SlidesDocumento46 páginasNursing Care of The Community: Control of Communicable Diseases Instructional SlidesJullienne Ysabelle AngAinda não há avaliações
- Diphtheria Pertussis TetanusDocumento43 páginasDiphtheria Pertussis Tetanuspnalinl108Ainda não há avaliações
- Dermato Venerology ScienceDocumento11 páginasDermato Venerology ScienceAQis AQishAinda não há avaliações
- Name: Carlo M. Yao Bachelor of Science in NursingDocumento33 páginasName: Carlo M. Yao Bachelor of Science in Nursingcarlo24_briggsAinda não há avaliações
- Infectious Diseases GuideDocumento30 páginasInfectious Diseases GuideSarahAinda não há avaliações
- Lecture 27-Epizoonosis-Dr. Agnes Sri Siswati, SP - KK (K) (2020)Documento45 páginasLecture 27-Epizoonosis-Dr. Agnes Sri Siswati, SP - KK (K) (2020)jasmine amaliaAinda não há avaliações
- Communicable Disease Review MaterialDocumento43 páginasCommunicable Disease Review Materialrceponelas1127Ainda não há avaliações
- Brucellosis in NepalDocumento22 páginasBrucellosis in NepalBinayaAinda não há avaliações
- Agent Source/Mot IP POC S/S Therapeutic MGMT Complications Nurisng ConsiderationsDocumento13 páginasAgent Source/Mot IP POC S/S Therapeutic MGMT Complications Nurisng ConsiderationsKuennie SabalAinda não há avaliações
- Vaccine PreventableDocumento89 páginasVaccine PreventableMohammad Doctor CabdiraxmanAinda não há avaliações
- Zoonotic Diseases: by Rita NkiroteDocumento44 páginasZoonotic Diseases: by Rita NkiroteIsaac JumaAinda não há avaliações
- Lerelyn Case Reading4Documento53 páginasLerelyn Case Reading4Ma Lerelyn DatinguinooAinda não há avaliações
- Definition:: Pelvic Inflammatory Disease (Pid)Documento20 páginasDefinition:: Pelvic Inflammatory Disease (Pid)Malueth AnguiAinda não há avaliações
- Case Study in Micro-1Documento50 páginasCase Study in Micro-1Angie Cabanting BañezAinda não há avaliações
- Community Notes by DR - Khan Final-1Documento44 páginasCommunity Notes by DR - Khan Final-1Aqib IshaqAinda não há avaliações
- Locally Endemic Diseases ControlhandoutDocumento3 páginasLocally Endemic Diseases ControlhandoutEshiebel OrganistaAinda não há avaliações
- Sexual Transmitted InfectionsDocumento44 páginasSexual Transmitted InfectionsDeshielanny AlagumolyAinda não há avaliações
- Vector Born Disease Organism and Infective AgentsDocumento31 páginasVector Born Disease Organism and Infective AgentsKhadeeja Abdul VaheedAinda não há avaliações
- Lecture On MEASLESDocumento16 páginasLecture On MEASLESNicole Villanueva, BSN - Level 3AAinda não há avaliações
- Medicine DENGUE EBOLA INFLUENZA SMALLPOXDocumento6 páginasMedicine DENGUE EBOLA INFLUENZA SMALLPOXMiguel MansillaAinda não há avaliações
- Communicable Diseasesp.170 199Documento30 páginasCommunicable Diseasesp.170 199Gary Largosa GallardoAinda não há avaliações
- Inflammatory & Immunologic Diseases IIIDocumento252 páginasInflammatory & Immunologic Diseases IIIiamaldrinoAinda não há avaliações
- FlipchartDocumento24 páginasFlipchartSamantha Ishi LimAinda não há avaliações
- Chickenpox 160531062051 PDFDocumento16 páginasChickenpox 160531062051 PDFJu Lie AnnAinda não há avaliações
- Lec. 2 - Pertusis and VaricellaDocumento14 páginasLec. 2 - Pertusis and VaricellaMy StoryAinda não há avaliações
- CHN - Communicable DiseaseDocumento117 páginasCHN - Communicable DiseaseGetom NgukirAinda não há avaliações
- Mumps ParotitisDocumento28 páginasMumps ParotitisShari' Si WahyuAinda não há avaliações
- NCM109 - Reviewer-Lp-1-To-Lp-4Documento54 páginasNCM109 - Reviewer-Lp-1-To-Lp-4princessAinda não há avaliações
- Circulatory System Infectious Diseases: Dengue Hemorrhagic Shock SyndromeDocumento3 páginasCirculatory System Infectious Diseases: Dengue Hemorrhagic Shock Syndromegrazelantonette.calubAinda não há avaliações
- A. Infectious ProcessDocumento22 páginasA. Infectious ProcessKyla Malapit GarvidaAinda não há avaliações
- Syphilis "The Great Pretender": By: Bruce MartinDocumento28 páginasSyphilis "The Great Pretender": By: Bruce MartinChatie PipitAinda não há avaliações
- Coronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowNo EverandCoronavirus Crisis: Information and Help in the 2020 Pandemic - What Everyone Should KnowAinda não há avaliações
- University of The Philippines Manila Palo, LeyteDocumento27 páginasUniversity of The Philippines Manila Palo, LeyteAbigail BrillantesAinda não há avaliações
- Blood Transfusion: Andrew Isiah P. Bonifacio, RNDocumento27 páginasBlood Transfusion: Andrew Isiah P. Bonifacio, RNAbigail BrillantesAinda não há avaliações
- Head Nurse Experience (Staffing)Documento3 páginasHead Nurse Experience (Staffing)Abigail BrillantesAinda não há avaliações
- Case Presentation (Ortho Ward) :: Pathophysiology of FractureDocumento2 páginasCase Presentation (Ortho Ward) :: Pathophysiology of FractureAbigail BrillantesAinda não há avaliações
- Family Nursing ProcessDocumento16 páginasFamily Nursing ProcessAbigail BrillantesAinda não há avaliações
- Assessing The NailsDocumento1 páginaAssessing The NailsAbigail BrillantesAinda não há avaliações
- Assessing The Mouth and Oropharynx Performance:: Lips and Buccal MucosaDocumento3 páginasAssessing The Mouth and Oropharynx Performance:: Lips and Buccal MucosaAbigail BrillantesAinda não há avaliações
- 1 Apgar and MMDST 1Documento34 páginas1 Apgar and MMDST 1Abigail BrillantesAinda não há avaliações
- Assessing The HairDocumento1 páginaAssessing The HairAbigail BrillantesAinda não há avaliações
- Assessing The Skull and Face PerformanceDocumento1 páginaAssessing The Skull and Face PerformanceAbigail BrillantesAinda não há avaliações
- Assessment of Head and NailsDocumento2 páginasAssessment of Head and NailsAbigail BrillantesAinda não há avaliações
- 2 ADLs 1Documento15 páginas2 ADLs 1Abigail BrillantesAinda não há avaliações
- 1 Functional Assessment of An AdultDocumento63 páginas1 Functional Assessment of An AdultAbigail BrillantesAinda não há avaliações
- Guterbock Hittite MedicineDocumento6 páginasGuterbock Hittite MedicineTarek AliAinda não há avaliações
- XareltofinalDocumento2 páginasXareltofinalMuniba NasimAinda não há avaliações
- Sarms 1 - The Ultimate Guide To SarmsDocumento4 páginasSarms 1 - The Ultimate Guide To SarmsHumbert Gym ColombinaAinda não há avaliações
- What Is CelecoxibDocumento3 páginasWhat Is CelecoxibKevin LabbeikAinda não há avaliações
- Damolo, Jules Aldrich C. October 30, 2021 Bsit 1 Year Block - A Instructor: Jerson CamayDocumento3 páginasDamolo, Jules Aldrich C. October 30, 2021 Bsit 1 Year Block - A Instructor: Jerson CamayAldrich Dos DamoloAinda não há avaliações
- Thorax and Lungs SGDocumento2 páginasThorax and Lungs SGDestinee Caple100% (1)
- Choking and AspirationDocumento23 páginasChoking and AspirationAgni MubarokAinda não há avaliações
- Dental ChartingDocumento51 páginasDental ChartingXuan5550% (1)
- Soccer Programme U19 Pre in SeasonDocumento38 páginasSoccer Programme U19 Pre in SeasonJeffrey Peeko100% (1)
- Limfoma Kutis Pada Pasien Yang Semula Di DiagnosisDocumento34 páginasLimfoma Kutis Pada Pasien Yang Semula Di DiagnosisChris MulyoAinda não há avaliações
- Cesarean Surgical Techniques - GLOWMDocumento36 páginasCesarean Surgical Techniques - GLOWMOana BalintAinda não há avaliações
- Daftar Harga Pengujian Dan Kalibrasi Alat KesehatanDocumento3 páginasDaftar Harga Pengujian Dan Kalibrasi Alat KesehatanVIDYA VIRA PAKSYA PUTRAAinda não há avaliações
- (Godefroy Christian) Super Health PDFDocumento231 páginas(Godefroy Christian) Super Health PDFAlexandre Dantas100% (1)
- Forensic Reports and Testimony: A Guide To Effective CommunicationDocumento2 páginasForensic Reports and Testimony: A Guide To Effective CommunicationNorfolk JournalAinda não há avaliações
- Clinical Case Studies 2007 Townend 443 53Documento12 páginasClinical Case Studies 2007 Townend 443 53cioaca12Ainda não há avaliações
- Evolution of Leprosy ControlDocumento16 páginasEvolution of Leprosy ControlSanthosh KumarAinda não há avaliações
- Latihan Soal Procedure TextDocumento2 páginasLatihan Soal Procedure TextSuwari RisnawatiAinda não há avaliações
- Grafic AsistentiDocumento64 páginasGrafic AsistentibadeaAinda não há avaliações
- 2002 Solution-Focused Brief TherapyDocumento9 páginas2002 Solution-Focused Brief Therapymgnpni100% (1)
- Microscopic Examination of UrineDocumento89 páginasMicroscopic Examination of UrineLucia SurduAinda não há avaliações
- 1358453842.3856hematology Question BankDocumento182 páginas1358453842.3856hematology Question BankKay BristolAinda não há avaliações
- Biochemistry and Histocytochemistry Research DevelopmentsDocumento377 páginasBiochemistry and Histocytochemistry Research Developmentsfenrisulven2010100% (1)
- Name: Shafiq Ur Rahman Class No. 36 BSN Year-Iii, Semester-Vi Topic: "Reflection On Subject of Mental Health Nursing"Documento3 páginasName: Shafiq Ur Rahman Class No. 36 BSN Year-Iii, Semester-Vi Topic: "Reflection On Subject of Mental Health Nursing"Shafiq Ur RahmanAinda não há avaliações
- Point of CareDocumento5 páginasPoint of CareDaniela RochaAinda não há avaliações
- GMFMscoresheetDocumento6 páginasGMFMscoresheetAbdur RasyidAinda não há avaliações
- Angelman Syndrome - Identification and ManagementDocumento10 páginasAngelman Syndrome - Identification and ManagementFajar YuniftiadiAinda não há avaliações
- Care PlanDocumento4 páginasCare Planapi-217086261Ainda não há avaliações
- Human Biology Laboratory 4: Body Tissues and Organization List The 4 Tissue Types and Give A General Function: Pg. 40Documento4 páginasHuman Biology Laboratory 4: Body Tissues and Organization List The 4 Tissue Types and Give A General Function: Pg. 40bugyourselfAinda não há avaliações
- Concept Map 3 MM (Abdominal Pain)Documento2 páginasConcept Map 3 MM (Abdominal Pain)Matt McKinleyAinda não há avaliações
- Cardioversion of Atrial Fibrillation and AtrialDocumento13 páginasCardioversion of Atrial Fibrillation and AtrialLabontu IustinaAinda não há avaliações