Você também pode gostar
- Mother To Child Transmission HBVDocumento48 páginasMother To Child Transmission HBVAyu Andini Putri100% (1)
- Pediatric Hiv - Zambia.Documento59 páginasPediatric Hiv - Zambia.Linus PuleAinda não há avaliações
- National AIDS Control Programme: Debajani NayakDocumento66 páginasNational AIDS Control Programme: Debajani NayakGandimareiAinda não há avaliações
- Hepatitis B in Pregnancy PDFDocumento38 páginasHepatitis B in Pregnancy PDFAlsyAinda não há avaliações
- Consequences of Corruption On African Public Health System: 28 November 2009Documento23 páginasConsequences of Corruption On African Public Health System: 28 November 2009longanga DieseAinda não há avaliações
- Population PyramidDocumento1 páginaPopulation PyramidBALOGO TRISHA MARIEAinda não há avaliações
- ILRT Dr. Sarbani-1 PDFDocumento48 páginasILRT Dr. Sarbani-1 PDFdurgesh kumar100% (1)
- Hiv Conference 2019Documento45 páginasHiv Conference 2019Keletso NyathiAinda não há avaliações
- 1-3 Day 1 - Community As People Community Health NursingDocumento11 páginas1-3 Day 1 - Community As People Community Health NursingBea Dela CenaAinda não há avaliações
- Use of Z-Scores For The Classification of MalnutritionDocumento16 páginasUse of Z-Scores For The Classification of Malnutritionapi-381899667% (3)
- FindingsDocumento4 páginasFindingsAFRIZAL SHAHRIL MISRIAinda não há avaliações
- Program2 THN 2016Documento32 páginasProgram2 THN 2016leonardoAinda não há avaliações
- GPH Tutok Gamutan Davao OrientalDocumento3 páginasGPH Tutok Gamutan Davao Orientalrizza RiveraAinda não há avaliações
- Afghanistan - Education Equity Profile For Adolescent GirlsDocumento16 páginasAfghanistan - Education Equity Profile For Adolescent GirlssalamAinda não há avaliações
- Colorectal Cancer Screening in Alberta ...Documento23 páginasColorectal Cancer Screening in Alberta ...cydolusAinda não há avaliações
- Mathematics School Based AssessmentDocumento12 páginasMathematics School Based AssessmentKatrina RampersadAinda não há avaliações
- Child Nutrition: Darmono SSDocumento53 páginasChild Nutrition: Darmono SSKiky SuryaAinda não há avaliações
- National 2010 RAPID-Presidential Term PDFDocumento41 páginasNational 2010 RAPID-Presidential Term PDFLeyrra Paclibar DiduloAinda não há avaliações
- Seminar Epidemi HIV Indonesia - 10april2019 - C6Documento59 páginasSeminar Epidemi HIV Indonesia - 10april2019 - C6Eny VeronikaAinda não há avaliações
- SchoolidDocumento27 páginasSchoolidapi-392364749Ainda não há avaliações
- Determinants SAARCDocumento24 páginasDeterminants SAARCmititelualex1Ainda não há avaliações
- WHO-webinar Innovation Malaria EliminationDocumento20 páginasWHO-webinar Innovation Malaria EliminationAJ JaelaniAinda não há avaliações
- Breakfast Intake Among Children and Adolescents: United States, 2015-2018Documento8 páginasBreakfast Intake Among Children and Adolescents: United States, 2015-2018Ánh NguyễnAinda não há avaliações
- Diabetes Patient EducationDocumento96 páginasDiabetes Patient EducationbajaocAinda não há avaliações
- Standar EtikDocumento13 páginasStandar Etikmuhammad bagusAinda não há avaliações
- HTN Slide Deck NewDocumento27 páginasHTN Slide Deck NewChristy BerryAinda não há avaliações
- Local Public Health in Uncertain Times: Julie Morita, MD Commissioner Chicago Department of Public HealthDocumento39 páginasLocal Public Health in Uncertain Times: Julie Morita, MD Commissioner Chicago Department of Public HealthNational Press FoundationAinda não há avaliações
- Cancer and Risk of COVID-19 Through A General Community SurveyDocumento4 páginasCancer and Risk of COVID-19 Through A General Community SurveySimona VisanAinda não há avaliações
- Ferrè Et Al.Documento19 páginasFerrè Et Al.martinsmicaelribeiroAinda não há avaliações
- Data Analysis CIA - 1Documento6 páginasData Analysis CIA - 1Albert Davis 2027916Ainda não há avaliações
- Health and Nutritional Status of Filipino Adults, 20-59 Years OldDocumento32 páginasHealth and Nutritional Status of Filipino Adults, 20-59 Years OldJose Mari TrinidadAinda não há avaliações
- Review Article: Early Intervention and Nonpharmacological Therapy of Myopia in Young AdultsDocumento12 páginasReview Article: Early Intervention and Nonpharmacological Therapy of Myopia in Young AdultsvennieAinda não há avaliações
- Young Adult FertilityDocumento81 páginasYoung Adult FertilityKenny CastañedaAinda não há avaliações
- The Preliminary Findings of South Africa's Latest HIV Household SurveyDocumento4 páginasThe Preliminary Findings of South Africa's Latest HIV Household SurveyBhekisisa HealthAinda não há avaliações
- Smoking Adults PDFDocumento22 páginasSmoking Adults PDFJermeLou BaoAinda não há avaliações
- Page - NBB ResearchDocumento41 páginasPage - NBB ResearchToche DoceAinda não há avaliações
- Cohort Survival (S.Y. 2015 - 2016 To 2018 - 2019)Documento7 páginasCohort Survival (S.Y. 2015 - 2016 To 2018 - 2019)Mae LaglivaAinda não há avaliações
- (FINAL) Prof. Dr. Dr. Bambang Budi Siswanto, SPJP (K) - Understanding HF in IndonesiaDocumento32 páginas(FINAL) Prof. Dr. Dr. Bambang Budi Siswanto, SPJP (K) - Understanding HF in IndonesiaTicksAinda não há avaliações
- Midas Safety - NFO PresentationDocumento12 páginasMidas Safety - NFO PresentationAbbas NaqviAinda não há avaliações
- Gambaran Epid HIV IndonesiaDocumento32 páginasGambaran Epid HIV IndonesiaIsti'anah SururyAinda não há avaliações
- Expanded National Nutrition Survey: 2019 Results: Health and Nutritional Status of Filipino Adults, 20-59 Years OldDocumento61 páginasExpanded National Nutrition Survey: 2019 Results: Health and Nutritional Status of Filipino Adults, 20-59 Years Oldzvfvr95hrkAinda não há avaliações
- Relocation and Redevelopment of Municipal HallDocumento6 páginasRelocation and Redevelopment of Municipal HallJenny Rhose MallariAinda não há avaliações
- PN PDFDocumento59 páginasPN PDFAmit PatelAinda não há avaliações
- Group A PulsesDocumento30 páginasGroup A PulsesShravan N.V.Ainda não há avaliações
- MediCall - Nursing Informatics App Proposal PDFDocumento20 páginasMediCall - Nursing Informatics App Proposal PDFPaul MarloweAinda não há avaliações
- HepB BD Experiences-Final - GhanaDocumento10 páginasHepB BD Experiences-Final - GhanaadhikatamaAinda não há avaliações
- Pencegahan HivDocumento36 páginasPencegahan HivyaneemayAinda não há avaliações
- Tata Laksana Diabetes TerpaduDocumento74 páginasTata Laksana Diabetes TerpaduNovita Cahya PuspitasariAinda não há avaliações
- Acute Viral HepatitisDocumento76 páginasAcute Viral HepatitisSaurabh SagunAinda não há avaliações
- Degree Outcomes Statement 2022Documento11 páginasDegree Outcomes Statement 2022AubreyAinda não há avaliações
- Report COVID Clinical ManagmentDocumento70 páginasReport COVID Clinical ManagmentJeevan Emmanual JoyAinda não há avaliações
- Have Households Recovered Post 2008?Documento9 páginasHave Households Recovered Post 2008?pelusonietoaxelAinda não há avaliações
- Population Ecology - 53.6 Part I: Age Structure DiagramsDocumento4 páginasPopulation Ecology - 53.6 Part I: Age Structure DiagramsFIRE STAR OF DEATHAinda não há avaliações
- 2020 PIR Carmen Cebu FINALDocumento39 páginas2020 PIR Carmen Cebu FINALHRH CARMEN CEBUAinda não há avaliações
- The Barbados Drug Information Network: Findings From The 2017 & 2018 ReportsDocumento49 páginasThe Barbados Drug Information Network: Findings From The 2017 & 2018 Reportsterrod gangstaAinda não há avaliações
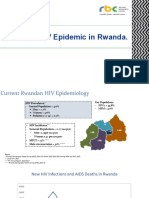
- State of HIV Epidemic in RwandaDocumento17 páginasState of HIV Epidemic in RwandaNshimiyimana Jean ClaudeAinda não há avaliações
- June 2006 QP - Paper 1 CIE Geography IGCSEDocumento16 páginasJune 2006 QP - Paper 1 CIE Geography IGCSERiskyRoadzAinda não há avaliações
- Development of Medical SectorDocumento24 páginasDevelopment of Medical SectorMahbubul Islam KoushickAinda não há avaliações
- Achieving the Demographic Dividend in the Arab Republic of Egypt: Choice, Not DestinyNo EverandAchieving the Demographic Dividend in the Arab Republic of Egypt: Choice, Not DestinyAinda não há avaliações
- Jl. DR. Sutomo No.16, Randusari, Kec. Semarang Selatan, Kota Semarang, Jawa Tengah 50244Documento6 páginasJl. DR. Sutomo No.16, Randusari, Kec. Semarang Selatan, Kota Semarang, Jawa Tengah 50244Muhammad FaisalAinda não há avaliações
- Twin Reversed Arterial Perfusion (TRAP) Sequence Characteristic Gray-Scale and Doppler Ultrasonography FindingsDocumento3 páginasTwin Reversed Arterial Perfusion (TRAP) Sequence Characteristic Gray-Scale and Doppler Ultrasonography FindingsMuhammad FaisalAinda não há avaliações
- Ogilvie SyndromeDocumento8 páginasOgilvie SyndromeMuhammad FaisalAinda não há avaliações
- COVID-19 Global Pandemic: Options For Management of Gynecologic CancersDocumento4 páginasCOVID-19 Global Pandemic: Options For Management of Gynecologic CancersMuhammad FaisalAinda não há avaliações
- Vaccines 09 00792Documento20 páginasVaccines 09 00792Muhammad FaisalAinda não há avaliações
- Unas November 2019Documento21 páginasUnas November 2019Muhammad FaisalAinda não há avaliações
- Berat Sebanding Dengan Meningkatnya Aktivitas Yang Dilakukan Oleh Manusia Khususnya Di Bidang Industri. Logam Kadmium Digunakan Di Berbagai Bidang SepertiDocumento8 páginasBerat Sebanding Dengan Meningkatnya Aktivitas Yang Dilakukan Oleh Manusia Khususnya Di Bidang Industri. Logam Kadmium Digunakan Di Berbagai Bidang SepertiMuhammad FaisalAinda não há avaliações
- Maternal Cadmium Levels During Pregnancy and The Relationship Wi 2018Documento8 páginasMaternal Cadmium Levels During Pregnancy and The Relationship Wi 2018Muhammad FaisalAinda não há avaliações
- Prevention of SSI - DR Aldika AkbarDocumento42 páginasPrevention of SSI - DR Aldika AkbarMuhammad FaisalAinda não há avaliações
- 1202 4509 1 PB PDFDocumento3 páginas1202 4509 1 PB PDFMuhammad FaisalAinda não há avaliações
- Soal Soal Obstetri WilliamDocumento1 páginaSoal Soal Obstetri WilliamMuhammad Faisal100% (1)
- Reproduction: Placental Markers of Folate-Related Metabolism in PreeclampsiaDocumento10 páginasReproduction: Placental Markers of Folate-Related Metabolism in PreeclampsiaMuhammad FaisalAinda não há avaliações
- Folate Metabolism Gene Polymorphisms MTHFR C677T and A1298C and Risk For Preeclampsia: A Meta-AnalysisDocumento9 páginasFolate Metabolism Gene Polymorphisms MTHFR C677T and A1298C and Risk For Preeclampsia: A Meta-AnalysisMuhammad FaisalAinda não há avaliações
- Genetics of Pre-Eclampsia and The Weight of Babies at Birth - Clinical and Genetic Studies in Sri LankaDocumento3 páginasGenetics of Pre-Eclampsia and The Weight of Babies at Birth - Clinical and Genetic Studies in Sri LankaMuhammad FaisalAinda não há avaliações
- Cummins Prem Blue 15w40 1-18 L Sing Ssv3028m18 Asia-Pacific Purple Book (GHS) - EnglishDocumento14 páginasCummins Prem Blue 15w40 1-18 L Sing Ssv3028m18 Asia-Pacific Purple Book (GHS) - EnglishjosephvanbacAinda não há avaliações
- ObamaDeception SupplementalBookletDocumento34 páginasObamaDeception SupplementalBookletAccurateHistorian100% (4)
- Magnetis Polus AmboDocumento4 páginasMagnetis Polus Amboadi.mititean1585Ainda não há avaliações
- 1.causes For Neonatal Sepsis, Newborn Sepsis, Neonatal Infection, Sepsis TreatmentDocumento12 páginas1.causes For Neonatal Sepsis, Newborn Sepsis, Neonatal Infection, Sepsis TreatmentlardiyahAinda não há avaliações
- Employee Benefits 6th Edition by Martocchio ISBN Solution ManualDocumento62 páginasEmployee Benefits 6th Edition by Martocchio ISBN Solution Manualbeverly100% (25)
- Fatimah Kti FixDocumento71 páginasFatimah Kti FixOktaviani MuhaddistAinda não há avaliações
- Campus Advocates: United Nations Association of The USADocumento10 páginasCampus Advocates: United Nations Association of The USAunausaAinda não há avaliações
- Manual of Homeopathic Practice (1876)Documento864 páginasManual of Homeopathic Practice (1876)Dr. JimAinda não há avaliações
- Uses of Isotopes in Our Daily LivesDocumento3 páginasUses of Isotopes in Our Daily LivesVibhor Mathur70% (10)
- 478 PeriodizationDocumento13 páginas478 Periodizationomarou1867% (3)
- Reflection Essay - HRM533Documento9 páginasReflection Essay - HRM533Mazatul NadirahAinda não há avaliações
- Spoon University Nutrition GuideDocumento80 páginasSpoon University Nutrition GuidermdelmandoAinda não há avaliações
- Freud's Psychosexual Stages of DevelopmentDocumento30 páginasFreud's Psychosexual Stages of DevelopmentjessaAinda não há avaliações
- Diabetes: Physical Activity and ExerciseDocumento2 páginasDiabetes: Physical Activity and ExerciseZobaida Khatun JulieAinda não há avaliações
- Magellan Code ChangesDocumento15 páginasMagellan Code ChangesdaringdreuAinda não há avaliações
- Spine Care Technologies Inc. and Zober Industries Inc. Announce Strategic AllianceDocumento3 páginasSpine Care Technologies Inc. and Zober Industries Inc. Announce Strategic AlliancePR.comAinda não há avaliações
- Patient Profile Patient Address Age Sex MaritalDocumento3 páginasPatient Profile Patient Address Age Sex Maritalunno hiquianaAinda não há avaliações
- Offshore Risk Management - Security Assessment For Offshore Oil PDFDocumento26 páginasOffshore Risk Management - Security Assessment For Offshore Oil PDFlightangeldavidAinda não há avaliações
- Msds CatDocumento7 páginasMsds CatraniAinda não há avaliações
- Glucose KitDocumento2 páginasGlucose KitJuan Enrique Ramón OrellanaAinda não há avaliações
- Migrants' Election ManifestoDocumento2 páginasMigrants' Election ManifestoMimi Panes - CorosAinda não há avaliações
- Tibetan Medicine and The CoronavirusDocumento1 páginaTibetan Medicine and The CoronavirusIvan IvanicAinda não há avaliações
- Facilities ManagementDocumento21 páginasFacilities ManagementEduardo Viana100% (1)
- Aetiology and Dlagnosis PDFDocumento21 páginasAetiology and Dlagnosis PDFFernaz BehlimAinda não há avaliações
- Summary of Chapters NFPA 1852: Standard On Selection, Care, and Maintenance of Open-Circuit Self-Contained Breathing Apparatus (SCBA)Documento2 páginasSummary of Chapters NFPA 1852: Standard On Selection, Care, and Maintenance of Open-Circuit Self-Contained Breathing Apparatus (SCBA)Rolando CerezoAinda não há avaliações
- IntroductionDocumento9 páginasIntroductionMarc Harold FloresAinda não há avaliações
- Stress and Coping Styles To StudentsDocumento8 páginasStress and Coping Styles To StudentsArien Kaye VallarAinda não há avaliações
- Filipino Research Paper Kabanata 4Documento8 páginasFilipino Research Paper Kabanata 4nynodok1pup3100% (1)
- 2019 EC 006 REORGANIZING BADAC Zone - 1Documento5 páginas2019 EC 006 REORGANIZING BADAC Zone - 1Barangay BotongonAinda não há avaliações
- Journal of Infection and Chemotherapy: Original ArticleDocumento7 páginasJournal of Infection and Chemotherapy: Original ArticleNoNWOAinda não há avaliações