Você também pode gostar
- OAB Treatment Center CopyrightDocumento60 páginasOAB Treatment Center CopyrightiamZebulunAinda não há avaliações
- Pancreatitis Group 3 NCM 116Documento21 páginasPancreatitis Group 3 NCM 116Diana Jane LauretaAinda não há avaliações
- Neurogenic BladderDocumento38 páginasNeurogenic Bladderminnalesri100% (1)
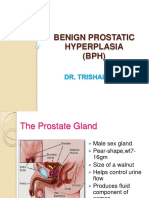
- Benign Prostatic HyperplasiaDocumento9 páginasBenign Prostatic Hyperplasiamardsz100% (1)
- Benign Prostatic Hyperplasia (BPH) : Free Nursing LecturesDocumento8 páginasBenign Prostatic Hyperplasia (BPH) : Free Nursing Lecturesmeshael_29Ainda não há avaliações
- Bladder Atony/Urinary RetentionDocumento11 páginasBladder Atony/Urinary RetentionAngela CaguitlaAinda não há avaliações
- Urinary IncontDocumento28 páginasUrinary Incontsayedmohammad mirlohiAinda não há avaliações
- Neurogenic Bladder (Ayurveda Co-Relation)Documento46 páginasNeurogenic Bladder (Ayurveda Co-Relation)Dr surendra A soniAinda não há avaliações
- Null - PDF 2Documento30 páginasNull - PDF 2مهند حسام محمد سعيد عبدAinda não há avaliações
- IncontinenceDocumento9 páginasIncontinenceHanaAinda não há avaliações
- MANAGING URINARY INCONTINENCE IN AGING PATIENTSDocumento34 páginasMANAGING URINARY INCONTINENCE IN AGING PATIENTSRetno Tri HaryatiAinda não há avaliações
- Benign Prostatic Hyperplasia (BPH)Documento70 páginasBenign Prostatic Hyperplasia (BPH)didiAinda não há avaliações
- Types and Treatment of Urinary Incontinence in WomenDocumento59 páginasTypes and Treatment of Urinary Incontinence in WomenAdnan WalidAinda não há avaliações
- Neurogenic Bladder Dysfunction: Mariano Marcos State UniversityDocumento6 páginasNeurogenic Bladder Dysfunction: Mariano Marcos State Universitychazney casianoAinda não há avaliações
- Urinary Incontinence: Genet Gebremedhin (MD) April 4 2017Documento34 páginasUrinary Incontinence: Genet Gebremedhin (MD) April 4 2017bemnetAinda não há avaliações
- Genuine Stress Incontinence Causes and TreatmentDocumento35 páginasGenuine Stress Incontinence Causes and TreatmentVeronica MendozaAinda não há avaliações
- Urogynecology and Pelvic ReconstructionDocumento28 páginasUrogynecology and Pelvic ReconstructionIKM FKUNSOEDAinda não há avaliações
- Motility Disorders 2Documento30 páginasMotility Disorders 2mohammed khalishAinda não há avaliações
- 3 - Neurogenic BladderDocumento14 páginas3 - Neurogenic Bladderanwar jabariAinda não há avaliações
- Care of Clients with Digestive and Absorption DisordersDocumento84 páginasCare of Clients with Digestive and Absorption DisordersKirstie Goc-ongAinda não há avaliações
- Benign Prostatic Hyperplasia. NCM 109Documento16 páginasBenign Prostatic Hyperplasia. NCM 109Niña Jean Tormis AldabaAinda não há avaliações
- URINARY INCONTINENCE: CAUSES AND EVALUATIONDocumento112 páginasURINARY INCONTINENCE: CAUSES AND EVALUATIONPrabhakar KumarAinda não há avaliações
- Types and Causes of Urinary IncontinenceDocumento9 páginasTypes and Causes of Urinary Incontinencehussain AltaherAinda não há avaliações
- Hirschsprung Disease (Congenital Aganglionic Megacolon) : By: Romeo Benjamin D. Laurente Group 4 BSN-2ADocumento11 páginasHirschsprung Disease (Congenital Aganglionic Megacolon) : By: Romeo Benjamin D. Laurente Group 4 BSN-2ARob Romeo Benjamin LaurenteAinda não há avaliações
- Overview of Urinary Incontinence (UI) in The Long Term Care FacilityDocumento81 páginasOverview of Urinary Incontinence (UI) in The Long Term Care Facilityالغزال الذهبيAinda não há avaliações
- Hyperemesis Gravidarum: Clinical Instructor: Ms. Ruby Ann B. Dimayuga, RN, MANDocumento19 páginasHyperemesis Gravidarum: Clinical Instructor: Ms. Ruby Ann B. Dimayuga, RN, MANR Hornilla ArcegaAinda não há avaliações
- CASE STUDY PPT Group1 - Revised WithoutvideoDocumento34 páginasCASE STUDY PPT Group1 - Revised WithoutvideoSamantha BolanteAinda não há avaliações
- Urinary Incontinence Cice 12 April 2017Documento43 páginasUrinary Incontinence Cice 12 April 2017deasyahAinda não há avaliações
- Urinary Incontinence in Elderly: DefinitionDocumento13 páginasUrinary Incontinence in Elderly: DefinitionTarek AhmedAinda não há avaliações
- CITICOLINE, Drugs in MedicalDocumento10 páginasCITICOLINE, Drugs in MedicalInosanto May AnnAinda não há avaliações
- Disorders of the Bladder and UrethraDocumento48 páginasDisorders of the Bladder and Urethralytonia dampeerAinda não há avaliações
- Term Paper On Nursing Pharmacology: Virgen Milagrosa University Foundation College of NursingDocumento13 páginasTerm Paper On Nursing Pharmacology: Virgen Milagrosa University Foundation College of NursingCharisse Joy CudalAinda não há avaliações
- 2ND To The Last SeshDocumento25 páginas2ND To The Last SeshnivraeAinda não há avaliações
- Constipation in ChildrenDocumento34 páginasConstipation in Childrenabdisalaan hassanAinda não há avaliações
- Fisilogi Anal KanalDocumento45 páginasFisilogi Anal KanalMargarethaAinda não há avaliações
- Urinary Incontinence: Dr. Sashmi Manandhar Department of Obstetrics and Gynaecology DH - KuhDocumento73 páginasUrinary Incontinence: Dr. Sashmi Manandhar Department of Obstetrics and Gynaecology DH - KuhSashmi ManandharAinda não há avaliações
- Uterostimulant and Relaxant 2Documento31 páginasUterostimulant and Relaxant 2Jefri SandikaAinda não há avaliações
- Irregular Bowel HabitDocumento66 páginasIrregular Bowel Habitfahim ahamedAinda não há avaliações
- Evaluation of The Incontinent Woman: Yeditepe University, Medical Faculty Dept of Ob&GynDocumento47 páginasEvaluation of The Incontinent Woman: Yeditepe University, Medical Faculty Dept of Ob&GynAdnan WalidAinda não há avaliações
- UI-Pharmacothrapy Handbook 11th Edition 2021Documento8 páginasUI-Pharmacothrapy Handbook 11th Edition 2021pbs4yvxjndAinda não há avaliações
- Neurogenic BlodderDocumento5 páginasNeurogenic BlodderBilal A AbdullahAinda não há avaliações
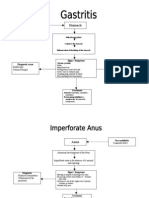
- Gastro PathophysiologyDocumento4 páginasGastro PathophysiologyPaul JoloAinda não há avaliações
- Urinary Incontinence Causes and TypesDocumento13 páginasUrinary Incontinence Causes and Typespreet kaurAinda não há avaliações
- Detrusor InstabilityDocumento7 páginasDetrusor Instabilityapi-3705046Ainda não há avaliações
- Types and Causes of Urinary IncontinenceDocumento13 páginasTypes and Causes of Urinary IncontinenceAshadeep KaurAinda não há avaliações
- Care for Urinary Problems & InfectionsDocumento7 páginasCare for Urinary Problems & InfectionsJosephine NavarroAinda não há avaliações
- Neurogenic BladderDocumento4 páginasNeurogenic BladderBonna PakerAinda não há avaliações
- Surgery - Female Urology and Incontinence (Tutorial)Documento6 páginasSurgery - Female Urology and Incontinence (Tutorial)halesAinda não há avaliações
- Types of Urinary IncontinenceDocumento1 páginaTypes of Urinary Incontinencehrg79qzwc2Ainda não há avaliações
- Uti, Incontinence, Neurogenic BladderDocumento3 páginasUti, Incontinence, Neurogenic Bladdermaan20Ainda não há avaliações
- Modul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaDocumento22 páginasModul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaYhaya 'Dzulhijjahyanti'Ainda não há avaliações
- Managing Benign Prostatic Hyperplasia (BPHDocumento9 páginasManaging Benign Prostatic Hyperplasia (BPHhussain Altaher0% (1)
- Manage Urinary Incontinence & RetentionDocumento13 páginasManage Urinary Incontinence & RetentionDeniela Jamaicy HerbertAinda não há avaliações
- The neuropathic lower urinary tractDocumento4 páginasThe neuropathic lower urinary tractBarez AminAinda não há avaliações
- Treatment and Testing of Stress Urinary IncontinenceDocumento52 páginasTreatment and Testing of Stress Urinary IncontinenceAlexandriah AlasAinda não há avaliações
- Conquering Incontinence: A new and physical approach to a freer lifestyleNo EverandConquering Incontinence: A new and physical approach to a freer lifestyleAinda não há avaliações
- Retrograde Ejaculation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandRetrograde Ejaculation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- Winning against Prostatitis in the Elderly. Insider’s View of a Medical Worker.No EverandWinning against Prostatitis in the Elderly. Insider’s View of a Medical Worker.Ainda não há avaliações
- Hip MaitlandDocumento14 páginasHip Maitlandakuphysio100% (1)
- Assist-1Documento25 páginasAssist-1akuphysioAinda não há avaliações
- Assistive Devices for AmbulationDocumento36 páginasAssistive Devices for Ambulationakuphysio100% (1)
- 12 Motor Control Approaches RDocumento26 páginas12 Motor Control Approaches R3520952Ainda não há avaliações
- SampleDocumento13 páginasSampleIrfan AhmedAinda não há avaliações
- Karachi Board Inter Date Sheet 2012Documento2 páginasKarachi Board Inter Date Sheet 2012akuphysioAinda não há avaliações
- Flow ChartDocumento3 páginasFlow Chartnitin235Ainda não há avaliações
- Physiotherapy and Orthopaedics: Internet Resources ForDocumento16 páginasPhysiotherapy and Orthopaedics: Internet Resources ForCindy Rara100% (1)
- Ventricular Peritoneal ShuntDocumento11 páginasVentricular Peritoneal ShuntakuphysioAinda não há avaliações
- Anderson4e Ch11 WithLectureNotesDocumento78 páginasAnderson4e Ch11 WithLectureNotesakuphysioAinda não há avaliações
- Makalah Gizi Dan Diet, Diet Penyakit GinjalDocumento38 páginasMakalah Gizi Dan Diet, Diet Penyakit GinjalRamadhani Riska Sucianti100% (1)
- Urinary IncontinenceDocumento1 páginaUrinary IncontinenceAinahMahaniAinda não há avaliações
- CystographyDocumento14 páginasCystographySuman PokhrelAinda não há avaliações
- What Is A Neobladder?Documento2 páginasWhat Is A Neobladder?WKYC.comAinda não há avaliações
- The Urinary SystemDocumento2 páginasThe Urinary SystemArl PasolAinda não há avaliações
- Gonorrhea Rates in the US from 1941-2007Documento16 páginasGonorrhea Rates in the US from 1941-2007Syasya NanaAinda não há avaliações
- Urology Case Reports: Aideen Madden, Asadullah Aslam, Nadeem B. NusratDocumento3 páginasUrology Case Reports: Aideen Madden, Asadullah Aslam, Nadeem B. NusratsoufiearyaniAinda não há avaliações
- Urinary Incontinence Guide for Care and ManagementDocumento5 páginasUrinary Incontinence Guide for Care and ManagementfakrulnersmudaAinda não há avaliações
- Distribution of CondomsDocumento8 páginasDistribution of CondomsMary Angelie CustodioAinda não há avaliações
- MS ObgyDocumento18 páginasMS ObgySushantaAinda não há avaliações
- Renal and Urinary Concept MapsDocumento8 páginasRenal and Urinary Concept Mapsnursing concept maps100% (1)
- Peer Review FormDocumento3 páginasPeer Review FormHitesh VermaAinda não há avaliações
- HealthDocumento103 páginasHealthLalita NaiduAinda não há avaliações
- Vaginal Discharge: By: Lisa Anggraeni Rizki FadillahDocumento12 páginasVaginal Discharge: By: Lisa Anggraeni Rizki FadillahRizkifadillahAinda não há avaliações
- Kidney stones: causes, symptoms and treatmentDocumento3 páginasKidney stones: causes, symptoms and treatmentSisti AninditaAinda não há avaliações
- Pediatric Robotic SurgeryDocumento188 páginasPediatric Robotic SurgeryPablo Lukacs CarmonaAinda não há avaliações
- Hubungan Management Cairan Dengan Tipe Sindrom Nefrotik Pada AnakDocumento6 páginasHubungan Management Cairan Dengan Tipe Sindrom Nefrotik Pada AnakTitis HandayaniAinda não há avaliações
- Reflex Facilitation: Vol Control of Micturition (Corticol Areas) Control EUS & Abd MDocumento1 páginaReflex Facilitation: Vol Control of Micturition (Corticol Areas) Control EUS & Abd MTharani KumaraAinda não há avaliações
- GonoraeDocumento16 páginasGonoraeOkta KendaAinda não há avaliações
- Inserting A Straight or Indwelling Catheter Catheterization - Is TheDocumento2 páginasInserting A Straight or Indwelling Catheter Catheterization - Is ThezjaneAinda não há avaliações
- Library - Sexuality Books - Calle Zorro - Shooting EjaculateDocumento37 páginasLibrary - Sexuality Books - Calle Zorro - Shooting EjaculateweyerAinda não há avaliações
- Pelvic Organ ProlapseDocumento5 páginasPelvic Organ Prolapsecgao30Ainda não há avaliações
- Male CircumcisionDocumento17 páginasMale CircumcisionSabera Kapasi100% (2)
- Lesson Plan UTIDocumento5 páginasLesson Plan UTITopeshwar TpkAinda não há avaliações
- Anatomy and PhysiologyDocumento5 páginasAnatomy and PhysiologyAica LupenaAinda não há avaliações
- Chapter 82 Urinary IncontinenceDocumento8 páginasChapter 82 Urinary IncontinenceNaronana AliAinda não há avaliações
- Penis: Abdomen Skin CircumcisionDocumento4 páginasPenis: Abdomen Skin CircumcisionTatadarz Auxtero LagriaAinda não há avaliações
- American Urological Association 2012 Meeting Exhibitor - ProspectusDocumento11 páginasAmerican Urological Association 2012 Meeting Exhibitor - ProspectusnicolaspharmaAinda não há avaliações
- Medical 1 PDFDocumento5 páginasMedical 1 PDFsuresh balajiAinda não há avaliações
- Urinary Ttract InfectionsDocumento20 páginasUrinary Ttract InfectionsmohamedomarabdelAinda não há avaliações