Você também pode gostar
- LipidsDocumento13 páginasLipidsalianaAinda não há avaliações
- Grape Seed Extract (Vitis Vinifera) Partially Reverses High Fat Diet-Induced Obesity in C57BL/6J MiceDocumento7 páginasGrape Seed Extract (Vitis Vinifera) Partially Reverses High Fat Diet-Induced Obesity in C57BL/6J MiceMohammad SutamiAinda não há avaliações
- Biochem Lec Term Paper HypoglycemiaDocumento8 páginasBiochem Lec Term Paper Hypoglycemiaapi-318284296Ainda não há avaliações
- Lipid and Glucose Methodology PDFDocumento16 páginasLipid and Glucose Methodology PDFJezzah Mae CañeteAinda não há avaliações
- SDLS 2008 Serum Total Protein and Albumin DeterminationDocumento2 páginasSDLS 2008 Serum Total Protein and Albumin DeterminationgenieqtAinda não há avaliações
- CH11-Amino Acid MetabolismDocumento106 páginasCH11-Amino Acid MetabolismChatchawinAinda não há avaliações
- Brothers: Integration of Metabolism and Metabolic Processes in Fed, Fasting and Starvation StatesDocumento14 páginasBrothers: Integration of Metabolism and Metabolic Processes in Fed, Fasting and Starvation StatesNischal DhAinda não há avaliações
- Biochemistry: Ihrevale LIPID META Bolism 1Documento92 páginasBiochemistry: Ihrevale LIPID META Bolism 1Roy BelenAinda não há avaliações
- Mode of Action: InsulinDocumento8 páginasMode of Action: Insulinmanus7777100% (1)
- Report EnzymesDocumento34 páginasReport Enzymesnestie villavirayAinda não há avaliações
- Glycoproteins: Charlotte V. Bañes, MDDocumento71 páginasGlycoproteins: Charlotte V. Bañes, MDswitimahaleAinda não há avaliações
- Lecture-5 Hormonal Regulation of Intestinal MotilityDocumento4 páginasLecture-5 Hormonal Regulation of Intestinal Motilityمرتضى حسين عبدAinda não há avaliações
- A Brief Overview of Hemoglobin ElectrophoresisDocumento46 páginasA Brief Overview of Hemoglobin Electrophoresisمجاهد إسماعيل حسن حسينAinda não há avaliações
- Tryptophan Metabolism: Dr. Ashok Kumar J International Medical School Management and Science University MalaysiaDocumento23 páginasTryptophan Metabolism: Dr. Ashok Kumar J International Medical School Management and Science University MalaysiaShah HuzaifaAinda não há avaliações
- B.D.S Course Biochemistry/Syllabus: (With Effect From 2010-11 Onwards)Documento4 páginasB.D.S Course Biochemistry/Syllabus: (With Effect From 2010-11 Onwards)AnandAinda não há avaliações
- Body FluidsDocumento24 páginasBody FluidsMohamed MidoAinda não há avaliações
- Introduction To Biochemistry: by Zaheer Uddin (Pharm-D, M Phil (Pharmacy Practice) MBA (MARKETING)Documento63 páginasIntroduction To Biochemistry: by Zaheer Uddin (Pharm-D, M Phil (Pharmacy Practice) MBA (MARKETING)Izat KhanAinda não há avaliações
- Written Exam Blue PrintDocumento12 páginasWritten Exam Blue PrintMotasim_mAinda não há avaliações
- Principles of Dna Isolation & PurificationDocumento10 páginasPrinciples of Dna Isolation & PurificationRatish Singh50% (2)
- Concise Biochemistry: Fundamental Principles: March 2016Documento52 páginasConcise Biochemistry: Fundamental Principles: March 2016Sagar DeshmaniAinda não há avaliações
- 2 - Lipid Metabolism Lecture For StudentsDocumento68 páginas2 - Lipid Metabolism Lecture For StudentshwhsgxAinda não há avaliações
- General Introduction and Basic Biochemical PrinciplesDocumento6 páginasGeneral Introduction and Basic Biochemical PrinciplescelecosibAinda não há avaliações
- 3dr Year Common Biochemistry MCQsDocumento8 páginas3dr Year Common Biochemistry MCQsYasmin Amr NounouAinda não há avaliações
- First Professional Mbbs Fourth Semester EXAMINATION SESSION-2007-2008 Subject - BiochemistryDocumento9 páginasFirst Professional Mbbs Fourth Semester EXAMINATION SESSION-2007-2008 Subject - BiochemistryIsrasami NaparAinda não há avaliações
- Git Biochemistry of GitDocumento9 páginasGit Biochemistry of GitSibatAinda não há avaliações
- Sphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeDocumento12 páginasSphingolipids: Dr. Abir Alghanouchi Biochemistry Department Sciences CollegeUzac BenuAinda não há avaliações
- Molecular CloningDocumento61 páginasMolecular CloningDavi DzikirianAinda não há avaliações
- 19.7 Membrane Lipids: Phospholipids: Group 3Documento36 páginas19.7 Membrane Lipids: Phospholipids: Group 3Masbateyeandlaser EyeclinicAinda não há avaliações
- Abnormal Constituents of UrineDocumento2 páginasAbnormal Constituents of UrineAries DocAinda não há avaliações
- Complex Carbohydrates - GlycoproteinsDocumento28 páginasComplex Carbohydrates - GlycoproteinsJessica SannohAinda não há avaliações
- Creatine and Creatinine MetabolismDocumento108 páginasCreatine and Creatinine MetabolismMae Matira AbeladorAinda não há avaliações
- Cholesterol - Synthesis, Metabolism, Regulation PDFDocumento10 páginasCholesterol - Synthesis, Metabolism, Regulation PDFAdreiTheTripleA100% (1)
- Protein SynthesisDocumento18 páginasProtein Synthesisabisantiago6131100% (1)
- ChromatographyDocumento31 páginasChromatographyarun231187Ainda não há avaliações
- Bioactive PeptidesDocumento16 páginasBioactive PeptidesOmotoyinbo SegunAinda não há avaliações
- Biochemistry of GlycoproteinDocumento6 páginasBiochemistry of GlycoproteinMahathir Mohmed100% (7)
- Diabetes Mellitus: Overview and TreatmentsDocumento36 páginasDiabetes Mellitus: Overview and TreatmentsGlenn Nadine N. Masicampo100% (1)
- Fatty Acid Synthesis 11.12.19Documento18 páginasFatty Acid Synthesis 11.12.19Sanreet Randhawa100% (1)
- PTT Body FluidsDocumento29 páginasPTT Body FluidsMalla Nova LayukAinda não há avaliações
- Purine & Pyrimidine MetabolismDocumento22 páginasPurine & Pyrimidine MetabolismManda100% (1)
- Biochem - (With Answers and Achievement Chart)Documento11 páginasBiochem - (With Answers and Achievement Chart)Valine Cysteine MethionineAinda não há avaliações
- Vitamins ReviewDocumento105 páginasVitamins Reviewjltrek123Ainda não há avaliações
- Metabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaDocumento60 páginasMetabolism of Carbohydrate: Department of Biochemistry Faculty of Medicine University of YARSI JakartaAmanda PutriAinda não há avaliações
- Glucose, Part1Documento33 páginasGlucose, Part1SarahAinda não há avaliações
- Clinical EnzymologyDocumento25 páginasClinical Enzymologyaminata6Ainda não há avaliações
- MCQ MembranesDocumento10 páginasMCQ MembranesMarilyne RizkAinda não há avaliações
- 2012-Fluid and ElectrolytesDocumento192 páginas2012-Fluid and ElectrolytesHarley Justiniani Dela CruzAinda não há avaliações
- Chapter 2 - Metabolism & Bioenergetics (Part 2) PDFDocumento69 páginasChapter 2 - Metabolism & Bioenergetics (Part 2) PDFdarren100% (2)
- Chemistryofproteinswithclinicalapplications 190621192525 PDFDocumento181 páginasChemistryofproteinswithclinicalapplications 190621192525 PDFAl-waleed Julkanain100% (1)
- Hexose Monophosphate ShuntDocumento43 páginasHexose Monophosphate ShuntSecret AgentAinda não há avaliações
- Biochemistry - C4 Proteins Determination of Primary StructureDocumento2 páginasBiochemistry - C4 Proteins Determination of Primary StructureKim LlamasAinda não há avaliações
- Porphyrias, Hemoglobinopathies and ThalassemiasDocumento11 páginasPorphyrias, Hemoglobinopathies and ThalassemiasGerald John PazAinda não há avaliações
- HMPDocumento44 páginasHMPraanja2Ainda não há avaliações
- Cells and Secretions of The Pancreatic IsletsDocumento4 páginasCells and Secretions of The Pancreatic IsletsSophia OcayAinda não há avaliações
- Cardiac MetabolismDocumento35 páginasCardiac Metabolismwaqas_xsAinda não há avaliações
- s15 Miller Chap 3b LectureDocumento25 páginass15 Miller Chap 3b LectureDorice Clement100% (1)
- Absorption of LipidsDocumento22 páginasAbsorption of LipidsEmm Noman100% (1)
- Ion TransportNo EverandIon TransportDavid KeelingAinda não há avaliações
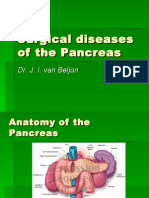
- SurgicalpancreasDocumento34 páginasSurgicalpancreasyasingadaAinda não há avaliações
- Drug AllergyDocumento117 páginasDrug AllergyyasingadaAinda não há avaliações
- General NosologyDocumento13 páginasGeneral Nosologyyasingada100% (1)
- Pathogenesis of Diseases. The Problem of Constitution Was OnlyDocumento4 páginasPathogenesis of Diseases. The Problem of Constitution Was OnlyyasingadaAinda não há avaliações
- 9 Metabolism of AAsDocumento25 páginas9 Metabolism of AAsyasingadaAinda não há avaliações
- Islamic MedicineDocumento20 páginasIslamic MedicineyasingadaAinda não há avaliações
- ATS2017 ProspectusDocumento13 páginasATS2017 ProspectusGiri WakshanAinda não há avaliações
- Research Methods in Developmental PsychologyDocumento9 páginasResearch Methods in Developmental PsychologyHugoAinda não há avaliações
- IbmautomtiveDocumento38 páginasIbmautomtiveMeltz NjorogeAinda não há avaliações
- Module 2 TechnologyDocumento20 páginasModule 2 Technologybenitez1Ainda não há avaliações
- Contemp Person Act.1Documento1 páginaContemp Person Act.1Luisa Jane De LunaAinda não há avaliações
- Lotus Exige Technical InformationDocumento2 páginasLotus Exige Technical InformationDave LeyAinda não há avaliações
- 02 Chapter 2 - Corporate Governance MechanismDocumento19 páginas02 Chapter 2 - Corporate Governance MechanismHanis ZahiraAinda não há avaliações
- Shaker ScreenDocumento2 páginasShaker ScreenRiaz EbrahimAinda não há avaliações
- MOS - Steel StructureDocumento15 páginasMOS - Steel StructuredennisAinda não há avaliações
- Arithmetic-Progressions - MDDocumento8 páginasArithmetic-Progressions - MDJay Jay GwizaAinda não há avaliações
- Nyambe African Adventures An Introduction To African AdventuresDocumento5 páginasNyambe African Adventures An Introduction To African AdventuresKaren LeongAinda não há avaliações
- Inspection Report For Apartment Building at 1080 93rd St. in Bay Harbor IslandsDocumento13 páginasInspection Report For Apartment Building at 1080 93rd St. in Bay Harbor IslandsAmanda RojasAinda não há avaliações
- DevOps Reference CardDocumento2 páginasDevOps Reference CardIntizarchauhanAinda não há avaliações
- Essay Final ProjectDocumento7 páginasEssay Final Projectapi-740591437Ainda não há avaliações
- Induction Motor Steady-State Model (Squirrel Cage) : MEP 1422 Electric DrivesDocumento21 páginasInduction Motor Steady-State Model (Squirrel Cage) : MEP 1422 Electric DrivesSpoiala DragosAinda não há avaliações
- Afzal ResumeDocumento4 páginasAfzal ResumeASHIQ HUSSAINAinda não há avaliações
- Cosmic Handbook PreviewDocumento9 páginasCosmic Handbook PreviewnkjkjkjAinda não há avaliações
- Introduction To AmplifierDocumento8 páginasIntroduction To AmplifierElaine BicolAinda não há avaliações
- Controlled DemolitionDocumento3 páginasControlled DemolitionJim FrancoAinda não há avaliações
- Donnan Membrane EquilibriaDocumento37 páginasDonnan Membrane EquilibriamukeshAinda não há avaliações
- DLI Watchman®: Vibration Screening Tool BenefitsDocumento2 páginasDLI Watchman®: Vibration Screening Tool Benefitssinner86Ainda não há avaliações
- Stochastic ProcessesDocumento264 páginasStochastic Processesmanosmill100% (1)
- Functions PW DPPDocumento4 páginasFunctions PW DPPDebmalyaAinda não há avaliações
- SahanaDocumento1 páginaSahanamurthyarun1993Ainda não há avaliações
- 7 ElevenDocumento80 páginas7 ElevenakashAinda não há avaliações
- Catalog Tu ZG3.2 Gian 35kV H'MunDocumento40 páginasCatalog Tu ZG3.2 Gian 35kV H'MunHà Văn TiếnAinda não há avaliações
- VLSI Implementation of Floating Point AdderDocumento46 páginasVLSI Implementation of Floating Point AdderParamesh Waran100% (1)
- Roland Fantom s88Documento51 páginasRoland Fantom s88harryoliff2672100% (1)
- LSL Education Center Final Exam 30 Minutes Full Name - Phone NumberDocumento2 páginasLSL Education Center Final Exam 30 Minutes Full Name - Phone NumberDilzoda Boytumanova.Ainda não há avaliações
- T688 Series Instructions ManualDocumento14 páginasT688 Series Instructions ManualKittiwat WongsuwanAinda não há avaliações