Você também pode gostar
- CPHQ Text BookDocumento20 páginasCPHQ Text BookCphq Cphq Ali100% (2)
- At4 886-12Documento110 páginasAt4 886-12scotty2hotty28100% (1)
- 9autacoids 14010v9023022 Phpapp02Documento109 páginas9autacoids 14010v9023022 Phpapp02h3cn1r3100% (1)
- Bars Performance AppraisalDocumento6 páginasBars Performance AppraisalPhillip Miler0% (1)
- Automobile Air Conditioning SystemDocumento8 páginasAutomobile Air Conditioning SystemAyyan Gaonkhadkar100% (1)
- ROA of AnimalsDocumento23 páginasROA of AnimalsMr.White sheep MusicAinda não há avaliações
- Routeadministration 4 PDFDocumento15 páginasRouteadministration 4 PDFLast StoryAinda não há avaliações
- Evaluation of Analgesic AgentsDocumento61 páginasEvaluation of Analgesic Agentsvasanth vijayAinda não há avaliações
- Mouse Handling Techniques PacketDocumento24 páginasMouse Handling Techniques PacketLovely Ann AyapanaAinda não há avaliações
- AntipyreticsDocumento5 páginasAntipyreticsClark LopezAinda não há avaliações
- Practice Pharmacology QuestionsDocumento34 páginasPractice Pharmacology QuestionsWilliam StaffAinda não há avaliações
- Diuretics Diuretics: Presentation By: DR Prabhakar Moderator: DR DamDocumento56 páginasDiuretics Diuretics: Presentation By: DR Prabhakar Moderator: DR DamPrabhakar KumarAinda não há avaliações
- Aiman - Patient Case Study ReportDocumento14 páginasAiman - Patient Case Study Reportezwan007100% (1)
- Micro Chart #3 - Italics OnlyDocumento27 páginasMicro Chart #3 - Italics Onlyapi-26938624100% (1)
- Protein Synthesis InhibitorsDocumento25 páginasProtein Synthesis InhibitorsSawsan Z. JwaiedAinda não há avaliações
- Normality N MolarityDocumento10 páginasNormality N Molaritynavigcp100% (9)
- Corticosteroids: Prof. Dr. Shah MuradDocumento51 páginasCorticosteroids: Prof. Dr. Shah MuradnehascribdjoshiAinda não há avaliações
- Challenges To Implementation of The Pharmaceutical Care Practice in Davao City.Documento11 páginasChallenges To Implementation of The Pharmaceutical Care Practice in Davao City.JessieLynMolinaAinda não há avaliações
- Indomethacin 392Documento17 páginasIndomethacin 392Mahadie Hasan JahadAinda não há avaliações
- Organisational Structure StudyDocumento49 páginasOrganisational Structure Studymiliya_abrahamAinda não há avaliações
- Indomethacin: By: Hedy Mae Bautista and Ana Francesca JacintoDocumento10 páginasIndomethacin: By: Hedy Mae Bautista and Ana Francesca JacintoAna FrancescaAinda não há avaliações
- Lab Techniques in MiceDocumento53 páginasLab Techniques in MiceSilverEva4Ainda não há avaliações
- AtropineDocumento14 páginasAtropineKrazygopa BalorAinda não há avaliações
- Chapter 1 Lecture Quality ControlDocumento23 páginasChapter 1 Lecture Quality ControlJudah Israel LescanoAinda não há avaliações
- AntidotesDocumento21 páginasAntidotesSandeep MahyavanshiAinda não há avaliações
- 61 80 Otc DrugsDocumento8 páginas61 80 Otc DrugsIra YaoAinda não há avaliações
- DiureticsDocumento49 páginasDiureticsamara cheemaAinda não há avaliações
- Introduction To Pharmacoepidemiology 2015 PDFDocumento20 páginasIntroduction To Pharmacoepidemiology 2015 PDFNovria Rizki HarahapAinda não há avaliações
- Antifungal Agent PPT PresentationDocumento38 páginasAntifungal Agent PPT Presentationdinberu tadesseAinda não há avaliações
- NSAIDSDocumento19 páginasNSAIDSDonna Kelly DuranAinda não há avaliações
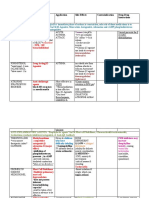
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocumento3 páginasDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinAinda não há avaliações
- Organoleptic TestingDocumento27 páginasOrganoleptic TestingmukhtarAinda não há avaliações
- Community Pharmacy Benchmarking Guideline 2011Documento33 páginasCommunity Pharmacy Benchmarking Guideline 2011omer tariqAinda não há avaliações
- Unit Operations in Secondary ManufacturingDocumento11 páginasUnit Operations in Secondary ManufacturingJoyce Marian BelonguelAinda não há avaliações
- Bronchodilator & Other Drugs Used in AsthmaDocumento15 páginasBronchodilator & Other Drugs Used in AsthmaGenta JagadAinda não há avaliações
- Gonadal Hormones and InhibitorsDocumento101 páginasGonadal Hormones and Inhibitors2012100% (4)
- Sulfonamides: By: Dr. Shruthi Rammohan Final Year PG Pharmacology RRMCHDocumento45 páginasSulfonamides: By: Dr. Shruthi Rammohan Final Year PG Pharmacology RRMCHAli Veer Ali VeerAinda não há avaliações
- Collection of Blood Sample From Experimental AnimalsDocumento12 páginasCollection of Blood Sample From Experimental AnimalslovehopeAinda não há avaliações
- Total Quality Management in Pharmaceuticals PDFDocumento11 páginasTotal Quality Management in Pharmaceuticals PDFNarongchai PongpanAinda não há avaliações
- 47-Drug Acting On Skin and MucousDocumento3 páginas47-Drug Acting On Skin and MucousMuhammad Sarmad MalikAinda não há avaliações
- Practical 1-Far 161-FinishDocumento10 páginasPractical 1-Far 161-FinishZulkifli Khairuddin100% (1)
- Adverse Drug ReactionDocumento24 páginasAdverse Drug ReactionGopal pokhrelAinda não há avaliações
- K46 Pharmacology of Anthelminthics, Antiprotozoal, & Antimalaria (Farmakologi)Documento78 páginasK46 Pharmacology of Anthelminthics, Antiprotozoal, & Antimalaria (Farmakologi)ayapillaiAinda não há avaliações
- The Role of Hospital Pharmacist As PreceptorDocumento14 páginasThe Role of Hospital Pharmacist As PreceptorKlub 'Apoteker' IndonesiaAinda não há avaliações
- Paracetamol PDFDocumento49 páginasParacetamol PDFEhb90210Ainda não há avaliações
- Antibiotics: Means Against LifeDocumento13 páginasAntibiotics: Means Against Lifeshankul kumar100% (1)
- Antiretroviral Agents 2017Documento38 páginasAntiretroviral Agents 2017Iman SaksoukAinda não há avaliações
- 3 ConstipationDocumento18 páginas3 Constipationكسلان اكتب اسميAinda não há avaliações
- Allergic Rhinitis PDFDocumento3 páginasAllergic Rhinitis PDFdrbilalmunirAinda não há avaliações
- Exploratory Study of Self-Medication Practices Among StudentsDocumento5 páginasExploratory Study of Self-Medication Practices Among StudentsN SAinda não há avaliações
- Diuretics and Other Pharmacological ActivityDocumento8 páginasDiuretics and Other Pharmacological ActivityMohan KalaskarAinda não há avaliações
- Dr. Rathnakar U.P.: Departments of Pharmacology Kasturba Medical College, MangaloreDocumento26 páginasDr. Rathnakar U.P.: Departments of Pharmacology Kasturba Medical College, MangaloreDr.U.P.Rathnakar.MD.DIH.PGDHMAinda não há avaliações
- New Drug Development and Approval ProcessDocumento19 páginasNew Drug Development and Approval ProcessKristine Aubrey AlvarezAinda não há avaliações
- Abbreviation Meaning: AbdominalDocumento3 páginasAbbreviation Meaning: AbdominalMariel GentilesAinda não há avaliações
- AutacoidsDocumento38 páginasAutacoidsdrmayangAinda não há avaliações
- Lecture 1 PDFDocumento75 páginasLecture 1 PDFBasil Elbushra Ahmed DomiAinda não há avaliações
- Dr. Rathnakar U.P.: Department of Pharmacology Kasturba Medical College, MangaloreDocumento25 páginasDr. Rathnakar U.P.: Department of Pharmacology Kasturba Medical College, MangaloreDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Adrenocorticosteroids and Adrenocortical AntagonistsDocumento53 páginasAdrenocorticosteroids and Adrenocortical AntagonistsKetan PatelAinda não há avaliações
- ExcretionDocumento35 páginasExcretionHely PatelAinda não há avaliações
- Anthelmintic Introduction-Diethylcarbamazine CitrateDocumento2 páginasAnthelmintic Introduction-Diethylcarbamazine CitrateEric Frazad MagsinoAinda não há avaliações
- Nurse Orientation - NarcoticsDocumento25 páginasNurse Orientation - NarcoticsSalma MustafaAinda não há avaliações
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingNo EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováAinda não há avaliações
- Sistem Komunikasi Antar-Sel: Nervous System Endocrine System Immune SystemDocumento38 páginasSistem Komunikasi Antar-Sel: Nervous System Endocrine System Immune SystemtangkasAinda não há avaliações
- Premium Connections Catalogue ENGDocumento134 páginasPremium Connections Catalogue ENGsubzwarijAinda não há avaliações
- SurveyDocumento1 páginaSurveyJainne Ann BetchaidaAinda não há avaliações
- The Bitter Internal Drive of AppleDocumento7 páginasThe Bitter Internal Drive of AppleBon WambuaAinda não há avaliações
- Different Types of FermentationDocumento26 páginasDifferent Types of FermentationCats and DogAinda não há avaliações
- Behavior Modification: Presented By: Wajeeha Iqbal BS in Psychology, MS (SLP/T) Riphah College of Rehabilitation SciencesDocumento28 páginasBehavior Modification: Presented By: Wajeeha Iqbal BS in Psychology, MS (SLP/T) Riphah College of Rehabilitation Sciencesmazahir hussainAinda não há avaliações
- AlaTOP Allergy Screen OUS - IMMULITE 2000 Systems - Rev 21 DXDCM 09017fe98067cfcb-1645658153157Documento28 páginasAlaTOP Allergy Screen OUS - IMMULITE 2000 Systems - Rev 21 DXDCM 09017fe98067cfcb-1645658153157Pierre LavoisierAinda não há avaliações
- PW6101 ProgrammationDocumento44 páginasPW6101 ProgrammationCédric DekeyserAinda não há avaliações
- Vocabulary June v22Documento2 páginasVocabulary June v22Wiston TonwisAinda não há avaliações
- Material Safety Data Sheet Roto-Inject FluidDocumento5 páginasMaterial Safety Data Sheet Roto-Inject FluidQuintana JoseAinda não há avaliações
- Exp 4 Centrifugal CompressorDocumento11 páginasExp 4 Centrifugal CompressorFaris HamirAinda não há avaliações
- RBC Disorder BcqsDocumento68 páginasRBC Disorder BcqsMukhtiar AhmedAinda não há avaliações
- Leoline Installation and MaintenanceDocumento8 páginasLeoline Installation and MaintenanceFloorkitAinda não há avaliações
- Scooty PepDocumento1 páginaScooty PepYASHAinda não há avaliações
- Equipment Available From SJ Turbine Inc.: LM Package Parts LM Package Parts High VoltageDocumento59 páginasEquipment Available From SJ Turbine Inc.: LM Package Parts LM Package Parts High VoltageAnibal QuezadaAinda não há avaliações
- Bai Tap Anh 9 Tuan 19202122 - 2032023135013Documento21 páginasBai Tap Anh 9 Tuan 19202122 - 2032023135013Duy HoangAinda não há avaliações
- Zook Rupture Disc URADocumento2 páginasZook Rupture Disc URAmd_taheriAinda não há avaliações
- PiscicultureDocumento14 páginasPisciculturejisha26100% (1)
- Dan Zahavi Josef Parnas - Schizophrenic - Autism - Clinical - Phenomenology PDFDocumento6 páginasDan Zahavi Josef Parnas - Schizophrenic - Autism - Clinical - Phenomenology PDFAdelar Conceição Dos SantosAinda não há avaliações
- Subject: Invitation To Join As "Resource Speaker" On Our Seminar On Fire Prevention and Safety ConsciousnessDocumento6 páginasSubject: Invitation To Join As "Resource Speaker" On Our Seminar On Fire Prevention and Safety ConsciousnessRjay CadaAinda não há avaliações
- Big BazaarDocumento6 páginasBig BazaaraniketsangodcarAinda não há avaliações
- EN Ultra V Mini STP410S C54 UmhDocumento2 páginasEN Ultra V Mini STP410S C54 Umhjabt4568Ainda não há avaliações
- Blotter EntryDocumento2 páginasBlotter EntryCharline Khie Silvestra PortemCamposanoAinda não há avaliações
- User Manual 4372070Documento80 páginasUser Manual 4372070EDENILSON CORDEIROAinda não há avaliações
- Gardobond 24d Imu Sds Ver1Documento6 páginasGardobond 24d Imu Sds Ver1stuart3962Ainda não há avaliações
- CD Compre Exam 2 Key AnswerDocumento6 páginasCD Compre Exam 2 Key AnswerGrace LazaroAinda não há avaliações
- Jurnal Kasus Etikolegal Dalam Praktik KebidananDocumento13 páginasJurnal Kasus Etikolegal Dalam Praktik KebidananErni AnggieAinda não há avaliações