Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Kindergarten Physical Education LessonDocumento7 páginasKindergarten Physical Education Lessonapi-185987237Ainda não há avaliações
- Research ProposalDocumento6 páginasResearch ProposalAhmad NajjarAinda não há avaliações
- Human Factor QuizDocumento5 páginasHuman Factor QuizSherif AL-KammashAinda não há avaliações
- Special Series On Effects of Board Games On HealthDocumento7 páginasSpecial Series On Effects of Board Games On HealthGAME CORNAinda não há avaliações
- Webinar Lung CancerDocumento53 páginasWebinar Lung CancerJose Flores FernandezAinda não há avaliações
- How To Read A CTG: What Is Cardiotocography?Documento11 páginasHow To Read A CTG: What Is Cardiotocography?Rinothja RajaratnamAinda não há avaliações
- Cognitive Behavioral Guided Self Help For The Treatment Od Recurrent Binge EatingDocumento19 páginasCognitive Behavioral Guided Self Help For The Treatment Od Recurrent Binge EatingIsmael RodriguezAinda não há avaliações
- Paired Facial Treatment With 755nm Picosecond Laser With Diffractive Lens Array and 1060nm Laser Lipolysis of The Submentum - An Open-Label Prospective TriaDocumento7 páginasPaired Facial Treatment With 755nm Picosecond Laser With Diffractive Lens Array and 1060nm Laser Lipolysis of The Submentum - An Open-Label Prospective TriaErik BrooksAinda não há avaliações
- Case Presentation 3 DR Oscar Laryngitis TBDocumento33 páginasCase Presentation 3 DR Oscar Laryngitis TBmarajuu50% (2)
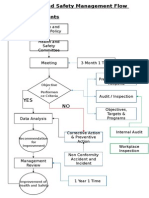
- Health and Safety FlowDocumento6 páginasHealth and Safety Flowzaki0304Ainda não há avaliações
- Systemic Review On The Use of Diclofenacb Complex As An Antiinflammatorytreatment With Pain Relief Effect For Patients With Acute Lower Back Pain 2167 0846 1000216Documento5 páginasSystemic Review On The Use of Diclofenacb Complex As An Antiinflammatorytreatment With Pain Relief Effect For Patients With Acute Lower Back Pain 2167 0846 1000216Dhea Yulia LubisAinda não há avaliações
- Crime Prevention LectureDocumento27 páginasCrime Prevention LectureCabagan IsabelaAinda não há avaliações
- COVID CertificateDocumento1 páginaCOVID CertificateshibiranAinda não há avaliações
- NCM 104 10 Herbal MedicinesDocumento4 páginasNCM 104 10 Herbal MedicinesElleAinda não há avaliações
- Online Class During PandemicDocumento6 páginasOnline Class During PandemicShariz DinoyoAinda não há avaliações
- FCA (SA) - Part - II - Past - Papers 7Documento29 páginasFCA (SA) - Part - II - Past - Papers 7matentenAinda não há avaliações
- Snapps PDFDocumento1 páginaSnapps PDFPatty Rivera100% (1)
- Challenges Facing People With Disabilities and Possible Solutions in TanzaniaDocumento8 páginasChallenges Facing People With Disabilities and Possible Solutions in TanzaniaKo ReaAinda não há avaliações
- 1 Script200302090903033030Documento9 páginas1 Script200302090903033030gever29816Ainda não há avaliações
- 2.2 NCM 109 - Complications During Pregnancy, Labor and Delivery and Postpartum PeriodsDocumento10 páginas2.2 NCM 109 - Complications During Pregnancy, Labor and Delivery and Postpartum PeriodsSittie Haneen TabaraAinda não há avaliações
- The Concept of Powerlessness in Patient Treatment Nursing EssayDocumento38 páginasThe Concept of Powerlessness in Patient Treatment Nursing EssayreginesulibAinda não há avaliações
- Management Hypovolemic Shock, NurinDocumento12 páginasManagement Hypovolemic Shock, Nurinرفاعي آكرمAinda não há avaliações
- 5 Minute Anxiety Relief TechniquesDocumento1 página5 Minute Anxiety Relief TechniquesBhettoh OrtizAinda não há avaliações
- Curahealth Hospitals Completes The Purchase of Specialty Hospital of JacksonvilleDocumento2 páginasCurahealth Hospitals Completes The Purchase of Specialty Hospital of JacksonvillePR.comAinda não há avaliações
- Branch Retinal Vein Occlusion (BRVO) : How Does BRVO Occur?Documento3 páginasBranch Retinal Vein Occlusion (BRVO) : How Does BRVO Occur?merizAinda não há avaliações
- P.E and Health ReviewerrDocumento14 páginasP.E and Health ReviewerrJoyce Anne Mae AdorioAinda não há avaliações
- Effect of Probiotics As A Complement To Non Surgical Periodontal Therapy in Chronic Periodontitis A Systematic RevieDocumento7 páginasEffect of Probiotics As A Complement To Non Surgical Periodontal Therapy in Chronic Periodontitis A Systematic RevieMohammedAinda não há avaliações
- Acute Gastroenteritis REPORTDocumento11 páginasAcute Gastroenteritis REPORTMelai Barneso Leal100% (1)
- Department of Labor: ls-210Documento1 páginaDepartment of Labor: ls-210USA_DepartmentOfLaborAinda não há avaliações
- Acute Flaccid Paralysis: Case Investigation FormDocumento2 páginasAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)