Você também pode gostar
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- Ma BruceiDocumento25 páginasMa Bruceiapi-3723461Ainda não há avaliações
- CVS VasodilatorsDocumento45 páginasCVS Vasodilatorsapi-3723461100% (1)
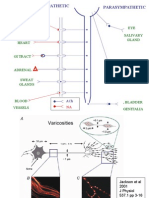
- Sympathetics EnglishDocumento72 páginasSympathetics Englishapi-3723461Ainda não há avaliações
- הרצאה 2- 29.5Documento51 páginasהרצאה 2- 29.5api-3723461Ainda não há avaliações
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Hipertension TranshemodialisisDocumento10 páginasHipertension TranshemodialisisMonica HerreraAinda não há avaliações
- Excretory System: Aceplukmannulhakim - Aula Hanim - Dheavannisa - EkajulianaDocumento48 páginasExcretory System: Aceplukmannulhakim - Aula Hanim - Dheavannisa - Ekajulianaaisyah mutiaraAinda não há avaliações
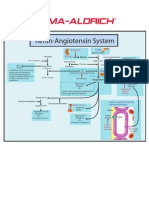
- Renin-Angiotensin SystemDocumento1 páginaRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Bazopril Is Legit (2023) Latest Updates!Documento1 páginaBazopril Is Legit (2023) Latest Updates!BazoprilBloodPressure SupportFormulaAinda não há avaliações
- Unit 06 Blood VesselsDocumento101 páginasUnit 06 Blood VesselsJohnykutty JosephAinda não há avaliações
- Blood Pressure RegulationDocumento11 páginasBlood Pressure RegulationManuAinda não há avaliações
- Nursing Drug CardsDocumento32 páginasNursing Drug CardsJenna Rasmussen100% (3)
- (The European Society of Cardiology) Rob Krams, Magnus Back - ESC TEXTBOOK of VASCULAR BIOLOGY (2017, Oxford University Press)Documento347 páginas(The European Society of Cardiology) Rob Krams, Magnus Back - ESC TEXTBOOK of VASCULAR BIOLOGY (2017, Oxford University Press)Muhammad AdithiaAinda não há avaliações
- Vasoactive PeptidesDocumento65 páginasVasoactive PeptidesJayrine MonteroAinda não há avaliações
- Pathophysiology and Etiology of Edema - IDocumento9 páginasPathophysiology and Etiology of Edema - IBrandy MaddoxAinda não há avaliações
- PreeclampsiaDocumento34 páginasPreeclampsiaCzyrine Tara EscoteAinda não há avaliações
- Management of Intradialytic Hypertension: The Ongoing ChallengeDocumento6 páginasManagement of Intradialytic Hypertension: The Ongoing ChallengeSari ChaerunisahAinda não há avaliações
- MCQ in PharmacyDocumento2 páginasMCQ in PharmacySwaroopSinghJakhar100% (1)
- Physiology Passmrcog 2016Documento73 páginasPhysiology Passmrcog 2016Mona HelouAinda não há avaliações
- Diagnosis and Treatment of HyperkalemiaDocumento9 páginasDiagnosis and Treatment of HyperkalemiaRoberto López MataAinda não há avaliações
- Fluid Management An Update For Perioperative PractitionersDocumento9 páginasFluid Management An Update For Perioperative PractitionersYuda PrawiraAinda não há avaliações
- Antihypertensive DrugsDocumento64 páginasAntihypertensive DrugsPSC100% (1)
- Case Study I2Documento48 páginasCase Study I2Emmanuel Andrew Dela CruzAinda não há avaliações
- PCOL - Chapter 11 - Anti Hypertensive AgentsDocumento3 páginasPCOL - Chapter 11 - Anti Hypertensive AgentsCharles BayogAinda não há avaliações
- Pathophysiology of HypertensionDocumento14 páginasPathophysiology of HypertensionRessy HastoprajaAinda não há avaliações
- Maternal Physiology During PregnancyDocumento28 páginasMaternal Physiology During PregnancyPutra MahautamaAinda não há avaliações
- The Raas: Renin ReleaseDocumento4 páginasThe Raas: Renin ReleaseAziil LiizaAinda não há avaliações
- Prostaglandins, Angiotensin and Bradikinin-Dr - Jibachha Sah, M.V.SC, LecturerDocumento27 páginasProstaglandins, Angiotensin and Bradikinin-Dr - Jibachha Sah, M.V.SC, Lecturerjibachha sahAinda não há avaliações
- Fluid Physiology 8.2 Infusion of Hypertonic SalineDocumento2 páginasFluid Physiology 8.2 Infusion of Hypertonic Salineicen00bAinda não há avaliações
- FLG 332 Renal Physiology - 1 (2019)Documento58 páginasFLG 332 Renal Physiology - 1 (2019)Huzaifa KhanAinda não há avaliações
- Calixtro, Narrative HypertensionDocumento2 páginasCalixtro, Narrative HypertensionKim SunooAinda não há avaliações
- Daily Practice AnswersDocumento37 páginasDaily Practice AnswersNazir AhmedAinda não há avaliações
- Cardiolog Y: Dian Paramita Kartikasari MAY, 17THDocumento51 páginasCardiolog Y: Dian Paramita Kartikasari MAY, 17THDian ParamitaAinda não há avaliações
- Anatomy & Physiology RenalDocumento27 páginasAnatomy & Physiology RenalMuchamad Wisuda RiswantoAinda não há avaliações
- ALISKIRENDocumento2 páginasALISKIRENLIEZEL GRACE VELAYOAinda não há avaliações