Você também pode gostar
- Week 5 CHNDocumento147 páginasWeek 5 CHNJelliAinda não há avaliações
- Epidemiology Week7 chn2 Aidavg Sept272020Documento131 páginasEpidemiology Week7 chn2 Aidavg Sept272020folkloriantaroAinda não há avaliações
- Questions For OSCE Exam - Model AnswersDocumento9 páginasQuestions For OSCE Exam - Model AnswersFarah FarahAinda não há avaliações
- Academic WritingDocumento48 páginasAcademic Writingسهى الغامديAinda não há avaliações
- Epidemiology: Dr. Siswanto, M.SCDocumento66 páginasEpidemiology: Dr. Siswanto, M.SCArinTa TyArlieAinda não há avaliações
- Questions For OSCE Exam - Model Answers 2Documento8 páginasQuestions For OSCE Exam - Model Answers 2Farah FarahAinda não há avaliações
- Chap 1 - Intro To Clinical EpidemiologyDocumento35 páginasChap 1 - Intro To Clinical Epidemiologybabyshaw76.sjAinda não há avaliações
- Module 1 Presentation For NotesDocumento31 páginasModule 1 Presentation For NotesRachaelAinda não há avaliações
- Epidemiologi Prof Bhisma MurtiDocumento32 páginasEpidemiologi Prof Bhisma MurtiniaasetaAinda não há avaliações
- 1st LectureDocumento6 páginas1st LectureNoreen FæţįmæAinda não há avaliações
- Crp5 k3 Prog PceDocumento33 páginasCrp5 k3 Prog PceAde IndrawanAinda não há avaliações
- Clinical Case Logs ReportDocumento14 páginasClinical Case Logs ReportSeth Therizwhiz RockerfellaAinda não há avaliações
- Introduction To Epidemiology Dr. Abdikani Ali MbbsDocumento38 páginasIntroduction To Epidemiology Dr. Abdikani Ali Mbbsabdikani hassanAinda não há avaliações
- Epidemiology: Dr. Siswanto, M.SCDocumento65 páginasEpidemiology: Dr. Siswanto, M.SCSharan SekhonAinda não há avaliações
- Lesson 5 Epidemiology and Public Health For Med Students 2022-2023Documento62 páginasLesson 5 Epidemiology and Public Health For Med Students 2022-2023salemAinda não há avaliações
- Questions For OSCE Exam - Model Answers 3Documento9 páginasQuestions For OSCE Exam - Model Answers 3Farah FarahAinda não há avaliações
- CHAPTER 4 Kelompok 3Documento45 páginasCHAPTER 4 Kelompok 3tri lestariAinda não há avaliações
- Epidemiology & Health Information: NU1103 Tara Brookes @tarapb8Documento40 páginasEpidemiology & Health Information: NU1103 Tara Brookes @tarapb8smartisaacAinda não há avaliações
- Epidemiology W1 - IntroductionDocumento24 páginasEpidemiology W1 - Introductionbalqis victoriaAinda não há avaliações
- Epidemiology: Assistant Professor Punjab University College of PharmacyDocumento20 páginasEpidemiology: Assistant Professor Punjab University College of PharmacyUsama AmjadAinda não há avaliações
- Questions For OSCE Exam 2Documento7 páginasQuestions For OSCE Exam 2Farah FarahAinda não há avaliações
- The Concept of Epidemiologic Surveillance: Ari UdijonoDocumento50 páginasThe Concept of Epidemiologic Surveillance: Ari UdijonoariAinda não há avaliações
- K-9 CRP 3.9 Epidemiologi KlinikDocumento27 páginasK-9 CRP 3.9 Epidemiologi KlinikJane Andrea Christiano DjianzonieAinda não há avaliações
- An Introduction To EpidemiologyDocumento27 páginasAn Introduction To Epidemiologyጀኔራል አሳምነው ፅጌAinda não há avaliações
- Acute Diarrheal Infections in AdultsDocumento21 páginasAcute Diarrheal Infections in AdultsNitiwut MeenunAinda não há avaliações
- Debre Markos University College of Health Science Department of Public Health Epidemiology For 2 Year BSC in Medical Laboratory Science Students by Mengistie Kassahun (MPH in Field Epidemiology)Documento55 páginasDebre Markos University College of Health Science Department of Public Health Epidemiology For 2 Year BSC in Medical Laboratory Science Students by Mengistie Kassahun (MPH in Field Epidemiology)Tewodros AntenehAinda não há avaliações
- Chapter 5 Epidemiology-CphDocumento51 páginasChapter 5 Epidemiology-CphMarcus Randielle FloresAinda não há avaliações
- CHN 2 NUR 1214 Week 2 Module 2.1Documento11 páginasCHN 2 NUR 1214 Week 2 Module 2.1Lorraine Jazmine AquinoAinda não há avaliações
- Study DesignsDocumento166 páginasStudy DesignsIsmail QamarAinda não há avaliações
- Introduction To Epidemiology2Documento59 páginasIntroduction To Epidemiology2Darlene Andres Ponce100% (1)
- EpidemiologyDocumento13 páginasEpidemiologyswethashaki50% (2)
- Maidul Lecture1Documento16 páginasMaidul Lecture1Arpita HalderAinda não há avaliações
- EpidemiologyDocumento20 páginasEpidemiologyho laAinda não há avaliações
- Module 4 Epidemiology and The Nurse (09182021)Documento28 páginasModule 4 Epidemiology and The Nurse (09182021)Ariane-Gay Cristobal DuranAinda não há avaliações
- What Is EpidemiologyDocumento19 páginasWhat Is EpidemiologyDfaid NG50% (2)
- PNADN010Documento6 páginasPNADN010Abdi MohammedAinda não há avaliações
- BANS-184 Important QuestionsDocumento31 páginasBANS-184 Important QuestionsRahul Singh RajputAinda não há avaliações
- Basic Concepts of EpidemiologyDocumento125 páginasBasic Concepts of EpidemiologyKailash Nagar100% (7)
- Epidemiology Principles and Methods Prof Bhisma MurtiDocumento32 páginasEpidemiology Principles and Methods Prof Bhisma Murtievy_silviania8873100% (1)
- Group 10Documento27 páginasGroup 10Carlmaigne Joy AgustinAinda não há avaliações
- Advance Epi & Direct Acyclic GraphDocumento14 páginasAdvance Epi & Direct Acyclic GraphPurnima VermaAinda não há avaliações
- PHR211Public Health: EpidemiologyDocumento59 páginasPHR211Public Health: EpidemiologyNuhu SibaAinda não há avaliações
- Methods Used in EpidemologyDocumento53 páginasMethods Used in EpidemologySameera banuAinda não há avaliações
- Epidemiology: Principles and Methods: Department of Public Health, Faculty of MedicineDocumento31 páginasEpidemiology: Principles and Methods: Department of Public Health, Faculty of MedicineFatwa Dea Ramdani OctaviyasminAinda não há avaliações
- LENS Introduction To PathophysiologyDocumento17 páginasLENS Introduction To PathophysiologyZyrille Moira MaddumaAinda não há avaliações
- Basic Concepts and Principles of EpidemiologyDocumento137 páginasBasic Concepts and Principles of EpidemiologyShubhamAinda não há avaliações
- MM20802-EPID IN CLINICAL PRACTICE Y2.v2Documento18 páginasMM20802-EPID IN CLINICAL PRACTICE Y2.v2danishAinda não há avaliações
- MPH 5103 Lecture 1 - 02092022 - ZTMDocumento38 páginasMPH 5103 Lecture 1 - 02092022 - ZTMRezwana SultanaAinda não há avaliações
- Screening: Dr. Win Khaing, PHD Associate ProfessorDocumento33 páginasScreening: Dr. Win Khaing, PHD Associate ProfessorWin KhaingAinda não há avaliações
- Epidemiology With Part 2 (Complete) 2Documento59 páginasEpidemiology With Part 2 (Complete) 2nahAinda não há avaliações
- Clinical EpidemiologyDocumento7 páginasClinical EpidemiologyMira Mariana UlfahAinda não há avaliações
- Epidemiology: By: Nosheen MustafaDocumento22 páginasEpidemiology: By: Nosheen MustafaMr.ShazAinda não há avaliações
- Epidemiology Principles and Methods Prof Bhisma MurtiDocumento32 páginasEpidemiology Principles and Methods Prof Bhisma MurtiMark Ian Caballes100% (1)
- MPH EocDocumento8 páginasMPH EocGalaleldin AliAinda não há avaliações
- Problem OneDocumento11 páginasProblem OnePei Qi LimAinda não há avaliações
- Principles of EpidemiologyDocumento5 páginasPrinciples of EpidemiologyJaffar ZabertAinda não há avaliações
- Reyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MDocumento50 páginasReyes, Kay Ma. Pearl Serranilla, Denisa Louise Tan, Francisco III Shivpura Sonia MGeraldine Marie Salvo100% (1)
- Epidemiological InterpretationDocumento9 páginasEpidemiological InterpretationKrishnaveni MurugeshAinda não há avaliações
- Epidemiology ADocumento18 páginasEpidemiology ABioquimica UplaAinda não há avaliações
- Case 14Documento7 páginasCase 14api-3743483100% (1)
- Case 16Documento6 páginasCase 16api-3743483Ainda não há avaliações
- Case 15Documento8 páginasCase 15api-3743483Ainda não há avaliações
- Case 12Documento8 páginasCase 12api-3743483Ainda não há avaliações
- Case 11Documento10 páginasCase 11api-3743483Ainda não há avaliações
- Case 13Documento7 páginasCase 13api-3743483Ainda não há avaliações
- Case 9 Algorithms)Documento4 páginasCase 9 Algorithms)api-3743483Ainda não há avaliações
- The Japanese ConnectionDocumento95 páginasThe Japanese Connectionapi-3743483100% (2)
- Rash JudgementDocumento54 páginasRash Judgementapi-3743483100% (1)
- Case 2 (Pgma-Rocklet-Wena-Manay-Chuchi-Pocha-Jb)Documento5 páginasCase 2 (Pgma-Rocklet-Wena-Manay-Chuchi-Pocha-Jb)api-3743483Ainda não há avaliações
- Case 9Documento10 páginasCase 9api-3743483100% (1)
- Case 3 (JB David Deo Glenn Cap)Documento5 páginasCase 3 (JB David Deo Glenn Cap)api-3743483Ainda não há avaliações
- Case 10Documento9 páginasCase 10api-3743483Ainda não há avaliações
- Case 1 (Manay Chuchi Pocha JB Deo Direk)Documento5 páginasCase 1 (Manay Chuchi Pocha JB Deo Direk)api-3743483Ainda não há avaliações
- Case 6Documento9 páginasCase 6api-3743483Ainda não há avaliações
- The Child With SeizureDocumento20 páginasThe Child With Seizureapi-3743483Ainda não há avaliações
- The Brain of The Blue BabyDocumento18 páginasThe Brain of The Blue Babyapi-3743483Ainda não há avaliações
- Shake Shake ShakeDocumento38 páginasShake Shake Shakeapi-3743483Ainda não há avaliações
- The Child With Motor Weakness 2Documento20 páginasThe Child With Motor Weakness 2api-3743483Ainda não há avaliações
- Machine Gun KellyDocumento30 páginasMachine Gun Kellyapi-3743483Ainda não há avaliações
- The Flight of The Lonely WandererDocumento30 páginasThe Flight of The Lonely Wandererapi-3743483Ainda não há avaliações
- The Child With Motor WeaknessDocumento22 páginasThe Child With Motor Weaknessapi-3743483Ainda não há avaliações
- Pesteng LamokDocumento13 páginasPesteng Lamokapi-3743483Ainda não há avaliações
- Mucocutaneous Symptom Complex Part 2Documento43 páginasMucocutaneous Symptom Complex Part 2api-3743483Ainda não há avaliações
- Wednesdays Child 2Documento72 páginasWednesdays Child 2api-3743483Ainda não há avaliações
- Kutis PorcelanaDocumento34 páginasKutis Porcelanaapi-3743483Ainda não há avaliações
- Kissin CousinsDocumento40 páginasKissin Cousinsapi-3743483Ainda não há avaliações
- Disease of The Seventh DayDocumento23 páginasDisease of The Seventh Dayapi-3743483Ainda não há avaliações
- Limping ChildDocumento23 páginasLimping Childapi-3743483Ainda não há avaliações
- What Is LeptospirosisDocumento9 páginasWhat Is LeptospirosisRotessa Joyce Diaz OngAinda não há avaliações
- Acute Abdomen (Modified From DR James Roring)Documento18 páginasAcute Abdomen (Modified From DR James Roring)Arga KafiAinda não há avaliações
- Icd 10 CM Pcs Coding Theory and Practice 2016 Edition 1st Edition Lovaasen Test BankDocumento11 páginasIcd 10 CM Pcs Coding Theory and Practice 2016 Edition 1st Edition Lovaasen Test Bankgisellephongejs100% (40)
- Health 8 - Q3 Module 1 V.1Documento14 páginasHealth 8 - Q3 Module 1 V.1cJ MalongAinda não há avaliações
- FIRST ANN - Booklet ROICAM 10Documento22 páginasFIRST ANN - Booklet ROICAM 10ssjjhrftbgAinda não há avaliações
- Secondary Data Analysis of ThiruvallurDocumento10 páginasSecondary Data Analysis of ThiruvallurSimbakutty VenkataramananAinda não há avaliações
- Lecture 9 Practice QuestionsDocumento13 páginasLecture 9 Practice QuestionslsatkinsAinda não há avaliações
- Study Desien - by Tahani AlghamdiDocumento41 páginasStudy Desien - by Tahani AlghamdiMian. Shoaib.Ainda não há avaliações
- Lesson 2 - Classification of DiseasesDocumento43 páginasLesson 2 - Classification of DiseasesHanis Joe100% (2)
- DISEASES - Immune SystemsDocumento3 páginasDISEASES - Immune SystemsMolan JenaAinda não há avaliações
- Negative: What Does It Mean To Have A Test Result?Documento2 páginasNegative: What Does It Mean To Have A Test Result?Todd EddyAinda não há avaliações
- Phenylketonur IA: Done byDocumento27 páginasPhenylketonur IA: Done byAsfoor gake1100% (1)
- Flight DocumentsDocumento1 páginaFlight DocumentsNguyen Thang LoiAinda não há avaliações
- E ColiDocumento8 páginasE Colihariprem26Ainda não há avaliações
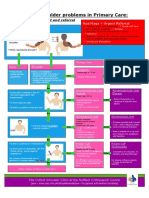
- NHS UK Diagnosis of Shoulder ProblemsDocumento1 páginaNHS UK Diagnosis of Shoulder ProblemsmertAinda não há avaliações
- Helen Lacey Seizures Draft1 29 Mar 2010Documento30 páginasHelen Lacey Seizures Draft1 29 Mar 2010Helen LaceyAinda não há avaliações
- Adrian Jess Galindo: DefinitionDocumento2 páginasAdrian Jess Galindo: DefinitionAdrian MangahasAinda não há avaliações
- Idx + Dengue Duo 52R2721AC-1Documento6 páginasIdx + Dengue Duo 52R2721AC-1antonio escobarAinda não há avaliações
- Kul 6 - Bias Dan Confounding Dalam EpidemiologiDocumento52 páginasKul 6 - Bias Dan Confounding Dalam EpidemiologibenzabensaaAinda não há avaliações
- Journal of The International AIDS Society - 2023 - Essajee - Getting Back On Track To Ending AIDS in Children It CouldDocumento2 páginasJournal of The International AIDS Society - 2023 - Essajee - Getting Back On Track To Ending AIDS in Children It Couldhalfani.solihAinda não há avaliações
- Yasay CHN Minor RequirementsDocumento6 páginasYasay CHN Minor RequirementsJoselo YasayAinda não há avaliações
- Biosecurity On Chicken FarmDocumento2 páginasBiosecurity On Chicken FarmBim ShiddiAinda não há avaliações
- Ecircular - 2876 - Announcement Extended Critical Illness (CI) CoverageDocumento5 páginasEcircular - 2876 - Announcement Extended Critical Illness (CI) Coveragechairkp 2015Ainda não há avaliações
- 10 General Symptoms of Hemochromatosis - Facty HealthDocumento3 páginas10 General Symptoms of Hemochromatosis - Facty HealthRosa AAinda não há avaliações
- REVISI (Adelita Setiawan 2)Documento7 páginasREVISI (Adelita Setiawan 2)Adelita SetiawanAinda não há avaliações
- Nclex Questions Chap 23 38Documento162 páginasNclex Questions Chap 23 38Sophia Rose Delos Santos100% (2)
- Case Scenerio Nephrotic SyndromeDocumento4 páginasCase Scenerio Nephrotic SyndromeEllen AngelAinda não há avaliações
- PATH Fit 2: Fitness Exercises Unit III: Risk Mitigation and ManagementDocumento20 páginasPATH Fit 2: Fitness Exercises Unit III: Risk Mitigation and ManagementKim GallegoAinda não há avaliações
- Infectious DeseasesDocumento16 páginasInfectious Deseaseslea jumawanAinda não há avaliações
- Regional Epidemiology Surveillance and Disaster Response UnitDocumento3 páginasRegional Epidemiology Surveillance and Disaster Response UnitthecutealAinda não há avaliações