Você também pode gostar
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (119)
- 52 Mutatie Brca Si Adn TerapieDocumento9 páginas52 Mutatie Brca Si Adn TerapieGabriela MilitaruAinda não há avaliações
- Guide to Selecting a Cooling Water Treatment ProgramDocumento2 páginasGuide to Selecting a Cooling Water Treatment ProgrammoncryAinda não há avaliações
- China GB4789.40 2010 Food Microbiological Examination Enterobacter Sakazakii PDFDocumento13 páginasChina GB4789.40 2010 Food Microbiological Examination Enterobacter Sakazakii PDFmmoradi55Ainda não há avaliações
- Implant Supported Overdenture: Presented By:-Dr. Anuja Gunjal 19/01/18Documento93 páginasImplant Supported Overdenture: Presented By:-Dr. Anuja Gunjal 19/01/18Instrument SeparationAinda não há avaliações
- PsychoanalysisDocumento30 páginasPsychoanalysisjaydokAinda não há avaliações
- Beat Brain FogDocumento19 páginasBeat Brain FogcarmenpaunAinda não há avaliações
- Tumor of The EyeDocumento30 páginasTumor of The EyenenyririAinda não há avaliações
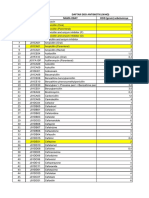
- DAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcDocumento12 páginasDAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcMahezha DhewaAinda não há avaliações
- DescargaDocumento173 páginasDescargaAlexander León PuelloAinda não há avaliações
- Indian Journal of Research in Pharmacy and Biotechnology (IJRPB) Vol-1 Issue-2Documento126 páginasIndian Journal of Research in Pharmacy and Biotechnology (IJRPB) Vol-1 Issue-2Debjit BhowmikAinda não há avaliações
- Philippine Nursing Code of Ethics and Patient's RightsDocumento17 páginasPhilippine Nursing Code of Ethics and Patient's RightsPauline M.Ainda não há avaliações
- Sepsis Guidelines: The Work of The Society of Critical Care MedicineDocumento3 páginasSepsis Guidelines: The Work of The Society of Critical Care MedicineRomina Zucco ZúñigaAinda não há avaliações
- Perioperative Venous ThromboembolismProphylaxiDocumento24 páginasPerioperative Venous ThromboembolismProphylaxiElías MendezAinda não há avaliações
- Clinical Psychology and PsychiatryDocumento10 páginasClinical Psychology and PsychiatryfoundationsAinda não há avaliações
- Therapeutics Handbook 2014 - 140804Documento384 páginasTherapeutics Handbook 2014 - 140804Eriet HidayatAinda não há avaliações
- Dharam Pani Pandey, Dr. Uday Shankar Sharma, Dr. Ram Babu. Electrical Muscle Stimulation (EMS) Improve Functional Independence in Critically Ill PatientsDocumento8 páginasDharam Pani Pandey, Dr. Uday Shankar Sharma, Dr. Ram Babu. Electrical Muscle Stimulation (EMS) Improve Functional Independence in Critically Ill PatientsDr. Krishna N. SharmaAinda não há avaliações
- Introduction To Clinical AssessmentDocumento13 páginasIntroduction To Clinical AssessmentnurmeenAinda não há avaliações
- Abordaje Linfadenopatia PerifericaDocumento13 páginasAbordaje Linfadenopatia PerifericaTony Gomez Luna LeyvaAinda não há avaliações
- Breast MassDocumento38 páginasBreast MassLester Paul SivilaAinda não há avaliações
- Hypnosis Tricks in Hindi PDFDocumento3 páginasHypnosis Tricks in Hindi PDFNavanath Damodar100% (1)
- FatigueDocumento8 páginasFatigueSabeeh Ul HassanAinda não há avaliações
- PHM Medisavers 2015 Insurance Policy SampleDocumento24 páginasPHM Medisavers 2015 Insurance Policy SampleNazim Saleh100% (1)
- Reflective QuestionsDocumento2 páginasReflective Questionsayne joulceAinda não há avaliações
- Parkinson DiseaseDocumento9 páginasParkinson DiseaseMarco GunawanAinda não há avaliações
- GI PathologyDocumento22 páginasGI Pathologyzeroun24100% (5)
- Kawasaki Disease Definition and DiagnosisDocumento3 páginasKawasaki Disease Definition and DiagnosisDavid ChengAinda não há avaliações
- Sample Practicum InternPlanDocumento5 páginasSample Practicum InternPlanNadz GimeAinda não há avaliações
- Host Modulation in Periodontics PDFDocumento12 páginasHost Modulation in Periodontics PDFCindyJessica100% (1)
- Principles in Trauma ManagementDocumento34 páginasPrinciples in Trauma Managementvirz23Ainda não há avaliações
- Disease Prevention Primary Secondary TertiaryDocumento1 páginaDisease Prevention Primary Secondary TertiaryprogramgrabberAinda não há avaliações