Você também pode gostar
- Diabetic KetoacidosisDocumento27 páginasDiabetic KetoacidosismrsotheaAinda não há avaliações
- Epidemiology and Management of Diarrheal DiseasesDocumento32 páginasEpidemiology and Management of Diarrheal DiseasesmrsotheaAinda não há avaliações
- Gout and PseudogoutDocumento113 páginasGout and PseudogoutmrsotheaAinda não há avaliações
- (Allred Charles) The GOUTDocumento23 páginas(Allred Charles) The GOUTmrsotheaAinda não há avaliações
- Clinical Formulary-Step TherapyDocumento21 páginasClinical Formulary-Step TherapymrsotheaAinda não há avaliações
- How To Start A New HospitalDocumento5 páginasHow To Start A New HospitalmrsotheaAinda não há avaliações
- Dka ChartDocumento2 páginasDka Chartmrsothea100% (1)
- Triage in Practice - A Random Is Ed ControlDocumento14 páginasTriage in Practice - A Random Is Ed ControlmrsotheaAinda não há avaliações
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Organization of The Human BodyDocumento6 páginasOrganization of The Human Bodysithum sanjanaAinda não há avaliações
- Fetal AbnormalitiesDocumento36 páginasFetal AbnormalitiesRaluca HabaAinda não há avaliações
- Abbreviations ListDocumento6 páginasAbbreviations ListolivedaisychainAinda não há avaliações
- Complete Blood CountDocumento3 páginasComplete Blood CountivantototaeAinda não há avaliações
- Cardio Pulmonary ResuscitationDocumento8 páginasCardio Pulmonary ResuscitationRuchika Kaushal71% (7)
- Instrucciones Fuente de Luz Olympus CLV-160Documento68 páginasInstrucciones Fuente de Luz Olympus CLV-160C J Ballesteros Montalbán100% (1)
- Option D (Postductal Coarctation of The Aorta) Is CorrectDocumento50 páginasOption D (Postductal Coarctation of The Aorta) Is Correctanimebests9Ainda não há avaliações
- 1 Practise Questions Keith Moore 5th Edition Should ReadDocumento113 páginas1 Practise Questions Keith Moore 5th Edition Should ReadNasan Shehada100% (1)
- BLS (Bantuan Hidup Dasar)Documento42 páginasBLS (Bantuan Hidup Dasar)Sam YahyaAinda não há avaliações
- Ncert Science NotesDocumento75 páginasNcert Science NotesRobin SharmaAinda não há avaliações
- 6 Thrombosis MorphologyDocumento20 páginas6 Thrombosis MorphologySawera RaheemAinda não há avaliações
- Anatomy Physiology Syllabus - LabDocumento7 páginasAnatomy Physiology Syllabus - Labapi-321286607Ainda não há avaliações
- Medicare Inpatient 2017Documento8.939 páginasMedicare Inpatient 2017Shashi Shirke100% (1)
- Facilitating Emotional Self Regulation in Preschool ChildrenDocumento36 páginasFacilitating Emotional Self Regulation in Preschool ChildrenIndra Daria100% (2)
- Mortality in Pop MusiciansDocumento38 páginasMortality in Pop MusiciansFran - Francesca ConfortiniAinda não há avaliações
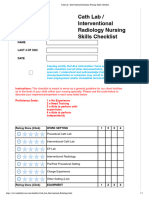
- Cath Lab - Interventional Radiology Nursing Skills ChecklistDocumento7 páginasCath Lab - Interventional Radiology Nursing Skills Checklistdk15janAinda não há avaliações
- Exchange Surfaces 1 QPDocumento12 páginasExchange Surfaces 1 QPSaaleh AbanurAinda não há avaliações
- 2011-2012 Annual Report Department of Pediatrics Saint Louis University School of MedicineDocumento131 páginas2011-2012 Annual Report Department of Pediatrics Saint Louis University School of Medicineslusompeds0% (1)
- Tens Vitalcontrol PDFDocumento20 páginasTens Vitalcontrol PDFOscar BravoAinda não há avaliações
- Acute Coronary Syndrome NCP 02Documento6 páginasAcute Coronary Syndrome NCP 02AgronaSlaughterAinda não há avaliações
- Module 8 - 50 MCQDocumento10 páginasModule 8 - 50 MCQAugene ToribioAinda não há avaliações
- Healthy Body Systems PowerPointDocumento42 páginasHealthy Body Systems PowerPointJianming WangAinda não há avaliações
- 2 Acute Myocardial InfarctionDocumento15 páginas2 Acute Myocardial InfarctionpauchanmnlAinda não há avaliações
- Chapter 37 Cardiac Glycosides Antianginals and AntidysrhythmicsDocumento5 páginasChapter 37 Cardiac Glycosides Antianginals and AntidysrhythmicsErika Joy Cabison TamayoAinda não há avaliações
- What Is Cardiovascular FitnessDocumento10 páginasWhat Is Cardiovascular FitnessAbigail AnziaAinda não há avaliações
- Physiologic Basis - Cardiopulmonary InteractionsDocumento4 páginasPhysiologic Basis - Cardiopulmonary InteractionsKatherine OhaAinda não há avaliações
- Structure of Human Heart-External FeaturesDocumento5 páginasStructure of Human Heart-External FeaturesAde Sintia DeviAinda não há avaliações
- Cardiac ArrhythmiaDocumento5 páginasCardiac ArrhythmiaDennis CobbAinda não há avaliações
- Irish Maternity Early Warning System (IMEWS)Documento27 páginasIrish Maternity Early Warning System (IMEWS)xxdrivexxAinda não há avaliações
- Cardiology WorkBookDocumento102 páginasCardiology WorkBookCastleKGAinda não há avaliações