Você também pode gostar
- Salter-Harris Fracture of The Proximal Humerus in An Adolescent GymnastDocumento1 páginaSalter-Harris Fracture of The Proximal Humerus in An Adolescent GymnastAbdel PérezAinda não há avaliações
- Regis Carpenter AAOMPT Poster 2008Documento1 páginaRegis Carpenter AAOMPT Poster 2008smokey73Ainda não há avaliações
- Effectiveness of Occupational Therapy in Rehabilitation of Guillain Barre Syndrome: A Case StudyDocumento4 páginasEffectiveness of Occupational Therapy in Rehabilitation of Guillain Barre Syndrome: A Case Studymuhammad didy supiani100% (1)
- CACHO NCP NeuromuscularDocumento3 páginasCACHO NCP NeuromuscularJaymee CachoAinda não há avaliações
- EffectivenessDocumento5 páginasEffectivenessHari25885Ainda não há avaliações
- The McKenzie Method Powerpoint 2008Documento57 páginasThe McKenzie Method Powerpoint 2008Marikit2012Ainda não há avaliações
- Effects of Low-Level Laser and PlyometriDocumento9 páginasEffects of Low-Level Laser and PlyometriHevin GokulAinda não há avaliações
- Manual Therapy RecoveryDocumento263 páginasManual Therapy RecoveryMfxMazprofxAinda não há avaliações
- 154 Chronic Sacroiliac JointDocumento7 páginas154 Chronic Sacroiliac JointpkrajniAinda não há avaliações
- Pembekalan BPI Sem 5Documento40 páginasPembekalan BPI Sem 5Mukhtar Ali MuktiAinda não há avaliações
- Shruti RamekarDocumento6 páginasShruti RamekarShruti RamekarAinda não há avaliações
- The McKenzie Method Powerpoint - 2008Documento57 páginasThe McKenzie Method Powerpoint - 2008aslooclt100% (2)
- The McKenzieDocumento57 páginasThe McKenzieStefan VladAinda não há avaliações
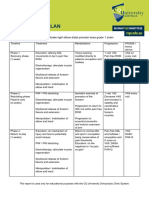
- Zac Williams Simple MSK Management PlanDocumento1 páginaZac Williams Simple MSK Management Planapi-468093714Ainda não há avaliações
- Cauda Equina Syndrome Secondary To Lumbar Disc Herniation. Report of Three CasesDocumento6 páginasCauda Equina Syndrome Secondary To Lumbar Disc Herniation. Report of Three CasesSugi WilliamAinda não há avaliações
- Activity Intolerance For CvaDocumento2 páginasActivity Intolerance For Cvalouie roderosAinda não há avaliações
- Regis WilsonAT AAOMPT Poster 2008Documento1 páginaRegis WilsonAT AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Thomas AAOMPT Poster 2008Documento1 páginaRegis Thomas AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Chovvath AAOMPT Poster 2008Documento1 páginaRegis Chovvath AAOMPT Poster 2008smokey73Ainda não há avaliações
- Cyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistDocumento44 páginasCyriax - Spine: by DR. Akshay A. Chougule (PT) Orthopaedic Manual TherapistAishwarya Shah100% (1)
- Case Report Rehabilitation Program in A Patient With Intertrochanteric Femoral FractureDocumento26 páginasCase Report Rehabilitation Program in A Patient With Intertrochanteric Femoral FractureNatalia LoredanaAinda não há avaliações
- Ni Et Al Compliment Ther Med, 22, 2014Documento8 páginasNi Et Al Compliment Ther Med, 22, 2014Ricardo Mourão AtorAinda não há avaliações
- 08 Lumbar Fusion PP OrthoDocumento17 páginas08 Lumbar Fusion PP Orthoapi-547492718Ainda não há avaliações
- Assessment: The Neurologic Exam: InterviewDocumento10 páginasAssessment: The Neurologic Exam: InterviewJun ManAinda não há avaliações
- Case Report Rehabilitation Program in A Patient With Bilateral Arthroplasty For Hip OsteoarthritisDocumento26 páginasCase Report Rehabilitation Program in A Patient With Bilateral Arthroplasty For Hip OsteoarthritisNatalia LoredanaAinda não há avaliações
- Cervical Radiculopathy Poster CDocumento1 páginaCervical Radiculopathy Poster Capi-302698660Ainda não há avaliações
- Manipulation and Selective Exercises Decrease Pelvic Anteversion and Low-Back Pain: A Pilot StudyDocumento4 páginasManipulation and Selective Exercises Decrease Pelvic Anteversion and Low-Back Pain: A Pilot StudyJorge De Araujo RochaAinda não há avaliações
- Exercise Therapy For Total Tear of Rotator Cuff: A Case ReportDocumento4 páginasExercise Therapy For Total Tear of Rotator Cuff: A Case ReportNovie AstiniAinda não há avaliações
- TBR Doktung LaveniaDocumento11 páginasTBR Doktung LaveniaRiaAinda não há avaliações
- Abstract ESPRMDocumento1 páginaAbstract ESPRMAdy LunguAinda não há avaliações
- Monday April 23, 2007 Volume 1, Issue 1Documento1 páginaMonday April 23, 2007 Volume 1, Issue 1api-26919768Ainda não há avaliações
- Physical Therapy Interventions in 68 Year Old Male With Trans-Femoral Amputation: A Case ReportDocumento6 páginasPhysical Therapy Interventions in 68 Year Old Male With Trans-Femoral Amputation: A Case ReportGisellaAinda não há avaliações
- 1 s2.0 S1877065714004072 MainDocumento1 página1 s2.0 S1877065714004072 MainGabriel Humberto Vásquez HerreraAinda não há avaliações
- Useof MC Kenziecervicalprotoco LDocumento7 páginasUseof MC Kenziecervicalprotoco LJigga mannAinda não há avaliações
- Danto AAO Convocation2012LectureDocumento48 páginasDanto AAO Convocation2012Lecturercastello20Ainda não há avaliações
- Table1: Option1 Option2 Option3 Option4 CorrectanswerDocumento24 páginasTable1: Option1 Option2 Option3 Option4 CorrectanswerSoom RamadanAinda não há avaliações
- Scienti Fic/Clinical Article: SciencedirectDocumento11 páginasScienti Fic/Clinical Article: SciencedirectRun CapAinda não há avaliações
- Cognitive Functional Therapy For TheDocumento13 páginasCognitive Functional Therapy For TheEma DanciuAinda não há avaliações
- Shockwave Treatment For Denerved MuscleDocumento6 páginasShockwave Treatment For Denerved MuscleMauricio PinalAinda não há avaliações
- MSK Pain LBPDocumento12 páginasMSK Pain LBPMd. Ariful IslamAinda não há avaliações
- Overview of Manual Therapy Assessment and Treatment of The Cervicothoracic SpineDocumento16 páginasOverview of Manual Therapy Assessment and Treatment of The Cervicothoracic SpineParakram Singh GaurAinda não há avaliações
- ScoliosesDocumento10 páginasScolioseschandiwalaAinda não há avaliações
- Case ReportDocumento14 páginasCase Reportapi-678217089Ainda não há avaliações
- Ra 2122204010014 Pooja Surve 17.9.21Documento23 páginasRa 2122204010014 Pooja Surve 17.9.21Pooja SurveAinda não há avaliações
- Frozen ShoulderDocumento4 páginasFrozen Shoulderjimitkapadia100% (1)
- Case Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureDocumento26 páginasCase Report Rehabilitation Program in A Patient With A Displaced Femoral Neck FractureNatalia LoredanaAinda não há avaliações
- Clinical Approach of Spinal Cord Injury Managament in Emergency SettingDocumento60 páginasClinical Approach of Spinal Cord Injury Managament in Emergency SettingSri Ariantini AriantiniAinda não há avaliações
- PTH 890 - Case Report Poster 1Documento1 páginaPTH 890 - Case Report Poster 1api-551757456Ainda não há avaliações
- University of Northern PhilippinesDocumento4 páginasUniversity of Northern PhilippinesJanelle Cabida SupnadAinda não há avaliações
- Protocolo Core ExaminationDocumento8 páginasProtocolo Core ExaminationBia DiasAinda não há avaliações
- NCPDocumento2 páginasNCPsphinx809100% (2)
- Nursing Care Plan - Spinal Cord InjuryDocumento2 páginasNursing Care Plan - Spinal Cord Injuryderic92% (36)
- Daftar Tilik APNDocumento17 páginasDaftar Tilik APNmarindadaAinda não há avaliações
- Group Pattern Muscle Activity Lower Back PainDocumento8 páginasGroup Pattern Muscle Activity Lower Back PainHossam BarghashAinda não há avaliações
- Case IcuDocumento5 páginasCase IcuTrisha SuazoAinda não há avaliações
- Low Back Pain and Muscles ActivityDocumento7 páginasLow Back Pain and Muscles Activitycris.endo.ceAinda não há avaliações
- Rotator Cuff Assessment PDFDocumento11 páginasRotator Cuff Assessment PDFMichele MarengoAinda não há avaliações
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesNo EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesNota: 1 de 5 estrelas1/5 (1)
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesNo EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesNota: 3.5 de 5 estrelas3.5/5 (3)
- Releasing the Rotator Cuff: A complete guide to freedom of the shoulderNo EverandReleasing the Rotator Cuff: A complete guide to freedom of the shoulderAinda não há avaliações
- Regis WilsonCGH AAOMPT Poster 2008Documento1 páginaRegis WilsonCGH AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Thomas AAOMPT Poster 2008Documento1 páginaRegis Thomas AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis WilsonAT AAOMPT Poster 2008Documento1 páginaRegis WilsonAT AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Overy AAOMPT Poster 2008Documento1 páginaRegis Overy AAOMPT Poster 2008smokey73100% (2)
- Regis McCracking AAOMPT Poster 2008Documento1 páginaRegis McCracking AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Mani AAOMPT Poster 2008Documento1 páginaRegis Mani AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Leal AAOMPT Poster 2008Documento1 páginaRegis Leal AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Garvey AAOMPT Poster 2008Documento1 páginaRegis Garvey AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Kirkland AAOMPT Poster 2008Documento1 páginaRegis Kirkland AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Koppenhaver AAOMPT Poster 2008Documento1 páginaRegis Koppenhaver AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis MacDonald AAOMPT Poster 2008Documento1 páginaRegis MacDonald AAOMPT Poster 2008smokey73Ainda não há avaliações
- Regis Chovvath AAOMPT Poster 2008Documento1 páginaRegis Chovvath AAOMPT Poster 2008smokey73Ainda não há avaliações
- Strength of Materials Aug 5 2017Documento16 páginasStrength of Materials Aug 5 2017MikaellaTeniolaAinda não há avaliações
- SwahiliDocumento7 páginasSwahiliMohammedAinda não há avaliações
- Demand, Elasticity of Demand and Demand ForecastingDocumento16 páginasDemand, Elasticity of Demand and Demand Forecastingankit thapliyal100% (1)
- Reflection PseudoscienceDocumento3 páginasReflection PseudoscienceSuganthi RamasamyAinda não há avaliações
- Ratio & Proportion Part 1Documento5 páginasRatio & Proportion Part 1P Singh KarkiAinda não há avaliações
- Resume Relevant CourseworkDocumento5 páginasResume Relevant Courseworkdkcvybifg100% (2)
- (Bible in History - La Bible Dans L'histoire 8) John T. Willis - Yahweh and Moses in Conflict - The Role of Exodus 4-24-26 in The Book of Exodus-Peter Lang International Academic Publishers (2010)Documento244 páginas(Bible in History - La Bible Dans L'histoire 8) John T. Willis - Yahweh and Moses in Conflict - The Role of Exodus 4-24-26 in The Book of Exodus-Peter Lang International Academic Publishers (2010)Anonymous s3LTiHpc8100% (2)
- Es PS 0614Documento6 páginasEs PS 0614陳相如Ainda não há avaliações
- Lescture OPACDocumento5 páginasLescture OPACAgulto, Ivan R.Ainda não há avaliações
- The Post OfficeDocumento4 páginasThe Post OfficeKatherine LuisAinda não há avaliações
- Onechanbara - Bikini Samurai Squad Game GuideDocumento83 páginasOnechanbara - Bikini Samurai Squad Game GuideStefan RoscaAinda não há avaliações
- Markets and Commodity Figures: Total Market Turnover StatisticsDocumento6 páginasMarkets and Commodity Figures: Total Market Turnover StatisticsTiso Blackstar GroupAinda não há avaliações
- Distortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaDocumento11 páginasDistortion of The Ecclesiological Views of Metropolitan Chrysostomos of PhlorinaHibernoSlavAinda não há avaliações
- Bob Dylan Diskografija Prevodi PesamaDocumento175 páginasBob Dylan Diskografija Prevodi PesamaJolanda NešovićAinda não há avaliações
- IFRS Session 1 To 3Documento40 páginasIFRS Session 1 To 3techna8Ainda não há avaliações
- Emcee Script For CompetitionDocumento2 páginasEmcee Script For CompetitionArdini Izzati100% (3)
- SPE 166182 Radio Frequency Identification (RFID) Leads The Way in The Quest For Intervention Free Upper Completion InstallationDocumento9 páginasSPE 166182 Radio Frequency Identification (RFID) Leads The Way in The Quest For Intervention Free Upper Completion InstallationjangolovaAinda não há avaliações
- 1.4 Creating Graphic OrganizerDocumento1 página1.4 Creating Graphic OrganizerTrixie Roselle Y. MesiasAinda não há avaliações
- Enga10 Speaking Test3Documento2 páginasEnga10 Speaking Test3luana serraAinda não há avaliações
- Melo V PeopleDocumento1 páginaMelo V PeoplejjangAinda não há avaliações
- ABC LTD ProposalDocumento4 páginasABC LTD ProposalAbhishek JurianiAinda não há avaliações
- This Study Resource WasDocumento2 páginasThis Study Resource Waskaye nicolasAinda não há avaliações
- Qualitative Research Chapter 1-5Documento16 páginasQualitative Research Chapter 1-5Mikhaela Centeno100% (1)
- Installing Hyperledger Fabric and Composer: Ser/latest/installing/development-To Ols - HTMLDocumento13 páginasInstalling Hyperledger Fabric and Composer: Ser/latest/installing/development-To Ols - HTMLVidhi jainAinda não há avaliações
- The Biography of Hazrat Shah Qamaos Sahib in One PageDocumento3 páginasThe Biography of Hazrat Shah Qamaos Sahib in One PageMohammed Abdul Hafeez, B.Com., Hyderabad, IndiaAinda não há avaliações
- Pale ExamDocumento4 páginasPale ExamPatrick Tan100% (1)
- Class 11 Assignment 10 (Prac)Documento3 páginasClass 11 Assignment 10 (Prac)9crollno14bhewensagarsahuAinda não há avaliações
- Dialogue-2: Problem of Our CountryDocumento6 páginasDialogue-2: Problem of Our CountrysiamAinda não há avaliações
- My Personal Brand and Career GoalsDocumento3 páginasMy Personal Brand and Career GoalsPhúc ĐàoAinda não há avaliações
- Types of Media and Media ConvergenceDocumento70 páginasTypes of Media and Media ConvergenceYsmile De LaraAinda não há avaliações