Você também pode gostar
- 03 Anal & Perianal DisordersDocumento56 páginas03 Anal & Perianal DisordersHafizah HoshniAinda não há avaliações
- 24 Anorectal ConditionsDocumento55 páginas24 Anorectal ConditionsRaisa CleizeraAinda não há avaliações
- Anal and Perianal ConditionsDocumento58 páginasAnal and Perianal ConditionsYonas YemidiralemAinda não há avaliações
- Recurrent UtiDocumento8 páginasRecurrent UtiRick Jeyrald AbagatAinda não há avaliações
- Complications of Parotid SurgeryDocumento22 páginasComplications of Parotid SurgeryAsline JesicaAinda não há avaliações
- Patient Positioning During AnaesthesiaDocumento6 páginasPatient Positioning During AnaesthesiaDarman ZulfikarAinda não há avaliações
- Collagen Stimulators in Body Applications A ReviewDocumento23 páginasCollagen Stimulators in Body Applications A Reviewvidianka rembulanAinda não há avaliações
- Shingles: by Samantha LucasDocumento12 páginasShingles: by Samantha LucassyafinazAinda não há avaliações
- Wound Dressing: Nor Afifi Syafika Binti Mohd NasirDocumento55 páginasWound Dressing: Nor Afifi Syafika Binti Mohd NasirlekhaAinda não há avaliações
- Hemorrhoids: Ginesha Hafidzy GarishahDocumento35 páginasHemorrhoids: Ginesha Hafidzy GarishahrizqinadiaAinda não há avaliações
- Examination of Chronic AbdomenDocumento43 páginasExamination of Chronic AbdomendrrajeshpsmsAinda não há avaliações
- Bleeding Per RectumeDocumento35 páginasBleeding Per RectumetharakaAinda não há avaliações
- Testicular TumorsDocumento42 páginasTesticular TumorsarhamAinda não há avaliações
- 328 Management of Polytrauma PatientDocumento62 páginas328 Management of Polytrauma PatientYanesh BishundatAinda não há avaliações
- Acute Trauma Care:: ShockDocumento45 páginasAcute Trauma Care:: ShockGeoffrey100% (1)
- Parathyroid Imaging - Preoperative Localisation Designed FinalDocumento38 páginasParathyroid Imaging - Preoperative Localisation Designed FinalPesonalattireAinda não há avaliações
- 10 EdemaDocumento23 páginas10 EdemaTalmaciu AmyAinda não há avaliações
- Venous DiseaseDocumento45 páginasVenous DiseaseNinch Nagac100% (1)
- Genital Surgical DiseasesDocumento18 páginasGenital Surgical DiseasesanojAinda não há avaliações
- Varian Cysts: The Lebanese Society of Obstetrics and GynecologyDocumento4 páginasVarian Cysts: The Lebanese Society of Obstetrics and GynecologyAde Gustina SiahaanAinda não há avaliações
- Kidney Stones - K.S. GopiDocumento4 páginasKidney Stones - K.S. GopiMahmood MuftiAinda não há avaliações
- Management of Acute and Chronic Retention in MenDocumento52 páginasManagement of Acute and Chronic Retention in MenSri HariAinda não há avaliações
- Urinary Tract Infection-AnthieDocumento25 páginasUrinary Tract Infection-AnthieGumarbio Setiadi ZakariaAinda não há avaliações
- Chapter 6 WoundhealingDocumento41 páginasChapter 6 WoundhealingMelba AlanoAinda não há avaliações
- Shingles PosterDocumento1 páginaShingles Posterapi-266804300100% (1)
- MeningitisDocumento6 páginasMeningitisCheena DolormenteAinda não há avaliações
- Post Op Assessment SurgeryDocumento20 páginasPost Op Assessment SurgeryAbdullah MatarAinda não há avaliações
- HemorrhoidsDocumento20 páginasHemorrhoidsEdwin PratamaAinda não há avaliações
- Urinary Tract Infections ChildrenDocumento26 páginasUrinary Tract Infections ChildrenNadia AmroAinda não há avaliações
- Healing and RepairDocumento44 páginasHealing and RepairHariharan DevarajAinda não há avaliações
- Differential Diagnosis Pain Right HypochondriumDocumento35 páginasDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- Kabwe Central Hospital KCH: Breast Cancer"Documento34 páginasKabwe Central Hospital KCH: Breast Cancer"Emmanuel MukukaAinda não há avaliações
- Skin TumorsDocumento56 páginasSkin TumorsAriba Asif100% (1)
- Skin and Subcutaneous TissueDocumento138 páginasSkin and Subcutaneous TissueNirav CHOVATIYAAinda não há avaliações
- Ulcers, Sinuses, FistulaDocumento13 páginasUlcers, Sinuses, FistulanelsonAinda não há avaliações
- Disorders of Parathyroid GlandsDocumento52 páginasDisorders of Parathyroid GlandsDr. Akash GuptaAinda não há avaliações
- Approach To A Patient With Jaundice: Group A9 Cho, Chua Family, Co Family, CofrerosDocumento115 páginasApproach To A Patient With Jaundice: Group A9 Cho, Chua Family, Co Family, CofrerosEunice Co100% (1)
- Cough: PHR Sangita ShakyaDocumento21 páginasCough: PHR Sangita ShakyaCurex QAAinda não há avaliações
- Umbilical HerniasDocumento10 páginasUmbilical HerniasDiana Jane LauretaAinda não há avaliações
- Chest IntubationDocumento42 páginasChest IntubationdrusmanjamilhcmdAinda não há avaliações
- Vascular Diseases (1 of 3)Documento4 páginasVascular Diseases (1 of 3)Doctor GeneralAinda não há avaliações
- 8.1b. Systole-Diastole & Cardiac CycleDocumento34 páginas8.1b. Systole-Diastole & Cardiac Cycleverysedatedx100% (1)
- Anatomy and Physiology of The SkinDocumento30 páginasAnatomy and Physiology of The SkinNancy VargasAinda não há avaliações
- EndocrineDocumento5 páginasEndocrineSundarajan ManiAinda não há avaliações
- Family Caregiver Guide TBIDocumento484 páginasFamily Caregiver Guide TBIZekel HealthcareAinda não há avaliações
- Hernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsDocumento43 páginasHernia: Inguinal - Surgical Anatomy, Presentation, Treatment, ComplicationsFobin VargheseAinda não há avaliações
- Assessing AbdomenDocumento115 páginasAssessing AbdomenKris TinaAinda não há avaliações
- PeritonitisDocumento19 páginasPeritonitisAditya SahidAinda não há avaliações
- Function of The SkinDocumento69 páginasFunction of The SkinapermatagamaAinda não há avaliações
- Urinary Tract InfectionDocumento24 páginasUrinary Tract InfectionraddagAinda não há avaliações
- Anorectal DiseasesDocumento15 páginasAnorectal DiseaseserickAinda não há avaliações
- Rotator Cuff TearsDocumento22 páginasRotator Cuff TearsTaufiq SuwardiAinda não há avaliações
- Salpingitis Pleno Minggu 2 Blok 3.1Documento10 páginasSalpingitis Pleno Minggu 2 Blok 3.1mustikaweniAinda não há avaliações
- Mal RotationDocumento13 páginasMal RotationkavyarkrnagarAinda não há avaliações
- UtiDocumento28 páginasUtiDrShweta SainiAinda não há avaliações
- Basic Principles of Wound ManagementDocumento14 páginasBasic Principles of Wound ManagementLuis RuizAinda não há avaliações
- l8 Management of Perianal Pain and ConditionsDocumento51 páginasl8 Management of Perianal Pain and ConditionsMohd Johari Mohd ShafuwanAinda não há avaliações
- Preseptor: Hj. Liza Nursanty, DR., Sp. B., M. Kes., FinacsDocumento30 páginasPreseptor: Hj. Liza Nursanty, DR., Sp. B., M. Kes., FinacsRosa NurkholidAinda não há avaliações
- Disorders of The Salivary Glands 2Documento109 páginasDisorders of The Salivary Glands 2ningappaAinda não há avaliações
- Incision and DrainageDocumento33 páginasIncision and DrainagemathisyncAinda não há avaliações
- Combined Shear and TensionDocumento16 páginasCombined Shear and TensionDAN MARK OPONDAAinda não há avaliações
- OurCatholicFaith PowerPoint Chapter1Documento21 páginasOurCatholicFaith PowerPoint Chapter1VinAinda não há avaliações
- Straight LineDocumento15 páginasStraight LineAyanAinda não há avaliações
- Sat Vocabulary Lesson and Practice Lesson 5Documento3 páginasSat Vocabulary Lesson and Practice Lesson 5api-430952728Ainda não há avaliações
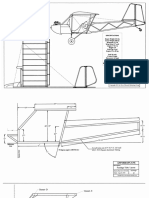
- Plans PDFDocumento49 páginasPlans PDFEstevam Gomes de Azevedo85% (34)
- Industrial Artificial Intelligence For Industry 4.0-Based Manufacturing SystemsDocumento5 páginasIndustrial Artificial Intelligence For Industry 4.0-Based Manufacturing SystemsMuhammad HaziqAinda não há avaliações
- Top Ten Myths About The BrainDocumento5 páginasTop Ten Myths About The BrainfayazalamaligAinda não há avaliações
- Effects of Climate ChangeDocumento3 páginasEffects of Climate Changejiofjij100% (1)
- American BreakfastDocumento4 páginasAmerican BreakfastHamilton Valenzuela ChipongianAinda não há avaliações
- The Passion For Cacti and Other Succulents: June 2017Documento140 páginasThe Passion For Cacti and Other Succulents: June 2017golf2010Ainda não há avaliações
- Niir Integrated Organic Farming Handbook PDFDocumento13 páginasNiir Integrated Organic Farming Handbook PDFNatalieAinda não há avaliações
- Main Girders: CrossDocumento3 páginasMain Girders: Crossmn4webAinda não há avaliações
- Scanner and Xcal Comperative Analysis v2Documento22 páginasScanner and Xcal Comperative Analysis v2Ziya2009Ainda não há avaliações
- 外贸专业术语Documento13 páginas外贸专业术语邱建华Ainda não há avaliações
- Sales 20: Years Advertising Expense (Millions) X Sales (Thousands) yDocumento8 páginasSales 20: Years Advertising Expense (Millions) X Sales (Thousands) ybangAinda não há avaliações
- Technical Information: Range-Free Controller FA-M3 System Upgrade GuideDocumento33 páginasTechnical Information: Range-Free Controller FA-M3 System Upgrade GuideAddaAinda não há avaliações
- IV. Network Modeling, Simple SystemDocumento16 páginasIV. Network Modeling, Simple SystemJaya BayuAinda não há avaliações
- Bulacan Agricultural State College: Lesson Plan in Science 4 Life Cycle of Humans, Animals and PlantsDocumento6 páginasBulacan Agricultural State College: Lesson Plan in Science 4 Life Cycle of Humans, Animals and PlantsHarmonica PellazarAinda não há avaliações
- Design and Development of Automatic Pneumatic Jack in Four Wheeler Ijariie5374Documento5 páginasDesign and Development of Automatic Pneumatic Jack in Four Wheeler Ijariie5374Saravanan ViswakarmaAinda não há avaliações
- Stepan Formulation 926Documento2 páginasStepan Formulation 926Moaz SiddigAinda não há avaliações
- Module 4 Active Faults and Other Earthquake Sources: Learning OutcomeDocumento3 páginasModule 4 Active Faults and Other Earthquake Sources: Learning OutcomeFatima Ybanez Mahilum-LimbagaAinda não há avaliações
- PEH Q3 Long QuizDocumento1 páginaPEH Q3 Long QuizBenedict LumagueAinda não há avaliações
- Indor Lighting DesignDocumento33 páginasIndor Lighting DesignRajesh MalikAinda não há avaliações
- 3rd Quarter Exam (Statistics)Documento4 páginas3rd Quarter Exam (Statistics)JERALD MONJUANAinda não há avaliações
- HCPL 316J 000eDocumento34 páginasHCPL 316J 000eElyes MbarekAinda não há avaliações
- Improve On-Time DeliveriesDocumento24 páginasImprove On-Time DeliveriesUdayAinda não há avaliações
- Curriculum Vitae - RadikaDocumento3 páginasCurriculum Vitae - RadikaradikahendryAinda não há avaliações
- Chapter 3.c (Centroid by Intergration)Documento15 páginasChapter 3.c (Centroid by Intergration)Ariff AziziAinda não há avaliações
- Irina Maleeva - Ariel Snowflake x6 - ENG - FreeDocumento4 páginasIrina Maleeva - Ariel Snowflake x6 - ENG - FreeMarinaKorzinaAinda não há avaliações
- Oil Whirl and Whip Instabilities - Within Journal BearingsDocumento27 páginasOil Whirl and Whip Instabilities - Within Journal BearingsTalha AamirAinda não há avaliações