Você também pode gostar
- ToxicologyDocumento76 páginasToxicologyAsma SikanderAinda não há avaliações
- Aeymon Atlas of Common EYE DiseasesDocumento140 páginasAeymon Atlas of Common EYE DiseasesAsma SikanderAinda não há avaliações
- ConstipationDocumento11 páginasConstipationAsma SikanderAinda não há avaliações
- History of TrigonometryDocumento10 páginasHistory of TrigonometryAsma SikanderAinda não há avaliações
- Id & Cs Material LogDocumento4 páginasId & Cs Material LogAsma SikanderAinda não há avaliações
- Kdigo-Gn-Guideline GN PDFDocumento143 páginasKdigo-Gn-Guideline GN PDFFerry JuniansyahAinda não há avaliações
- MRCP SyllabusDocumento145 páginasMRCP SyllabusCalvinAinda não há avaliações
- Short QDocumento53 páginasShort QAsma SikanderAinda não há avaliações
- Viral Hepatitis: Yonghong Zhang M.D. D.Phil. Beijing Youan Hospital Capital Medical UniversityDocumento41 páginasViral Hepatitis: Yonghong Zhang M.D. D.Phil. Beijing Youan Hospital Capital Medical UniversityAsma SikanderAinda não há avaliações
- SleDocumento893 páginasSleAsma Sikander100% (4)
- 异位妊娠2011Documento65 páginas异位妊娠2011Asma SikanderAinda não há avaliações
- 09 前置胎盘Documento87 páginas09 前置胎盘Asma SikanderAinda não há avaliações
- Hypertensive Disorders of PregnancyDocumento59 páginasHypertensive Disorders of PregnancyAsma SikanderAinda não há avaliações
- 1000 Prometric MCQ Solved 2Documento351 páginas1000 Prometric MCQ Solved 2chronos653490% (106)
- Paeds Outline1Documento13 páginasPaeds Outline1Asma SikanderAinda não há avaliações
- It Has Been My Experience That Maximizing Income Is A Helluva Lot Less Important Than Maximizing Passion and Fulfillment in Your Both Professionally and PersonallyDocumento1 páginaIt Has Been My Experience That Maximizing Income Is A Helluva Lot Less Important Than Maximizing Passion and Fulfillment in Your Both Professionally and PersonallyAsma SikanderAinda não há avaliações
- FilzaDocumento1 páginaFilzaAsma SikanderAinda não há avaliações
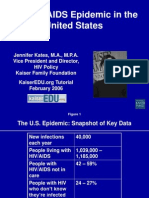
- The HIV/AIDS Epidemic in The United StatesDocumento27 páginasThe HIV/AIDS Epidemic in The United StatesAsma SikanderAinda não há avaliações
- F The Normal and Abnormal Transformation ZoneDocumento6 páginasF The Normal and Abnormal Transformation ZoneAsma SikanderAinda não há avaliações
- Hemorrhagic Fever With Renal Syndrome: Duan Zhongping MDDocumento68 páginasHemorrhagic Fever With Renal Syndrome: Duan Zhongping MDAsma SikanderAinda não há avaliações
- Medical Record 2Documento7 páginasMedical Record 2Asma SikanderAinda não há avaliações
- The HIV/AIDS Epidemic in The United StatesDocumento27 páginasThe HIV/AIDS Epidemic in The United StatesAsma SikanderAinda não há avaliações
- Viral Hepatitis: Yonghong Zhang M.D. D.Phil. Beijing Youan Hospital Capital Medical UniversityDocumento41 páginasViral Hepatitis: Yonghong Zhang M.D. D.Phil. Beijing Youan Hospital Capital Medical UniversityAsma SikanderAinda não há avaliações
- Chchinese 1Documento2 páginasChchinese 1Asma SikanderAinda não há avaliações
- NeuroDocumento3 páginasNeuroAsma SikanderAinda não há avaliações
- Examination On Infectious Diseases For Capital Medical University 200X Batch Overseas StudentsDocumento2 páginasExamination On Infectious Diseases For Capital Medical University 200X Batch Overseas StudentsAsma SikanderAinda não há avaliações
- New Microsoft Office Word DocumentDocumento2 páginasNew Microsoft Office Word DocumentAsma SikanderAinda não há avaliações
- Ricardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaDocumento20 páginasRicardo A. Caicedo, MD: Pediatric Gastroenterology University of FloridaAsma SikanderAinda não há avaliações
- 2 Cranialz and Sensory Motor and CaseDocumento90 páginas2 Cranialz and Sensory Motor and CaseAsma SikanderAinda não há avaliações
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNo EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeNota: 4 de 5 estrelas4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)No EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Nota: 4 de 5 estrelas4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNo EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryNota: 3.5 de 5 estrelas3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNo EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceNota: 4 de 5 estrelas4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingNo EverandThe Little Book of Hygge: Danish Secrets to Happy LivingNota: 3.5 de 5 estrelas3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItNo EverandNever Split the Difference: Negotiating As If Your Life Depended On ItNota: 4.5 de 5 estrelas4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNo EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureNota: 4.5 de 5 estrelas4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerNo EverandThe Emperor of All Maladies: A Biography of CancerNota: 4.5 de 5 estrelas4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnNo EverandTeam of Rivals: The Political Genius of Abraham LincolnNota: 4.5 de 5 estrelas4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNo EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaNota: 4.5 de 5 estrelas4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNo EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersNota: 4.5 de 5 estrelas4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyNo EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyNota: 3.5 de 5 estrelas3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNo EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreNota: 4 de 5 estrelas4/5 (1090)
- The Unwinding: An Inner History of the New AmericaNo EverandThe Unwinding: An Inner History of the New AmericaNota: 4 de 5 estrelas4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)No EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Nota: 4.5 de 5 estrelas4.5/5 (121)
- Tech SharmitDocumento16 páginasTech SharmitRishu SinhaAinda não há avaliações
- Appsc Aee Mains 2019 Electrical Engineering Paper III 1fcbb2c9Documento12 páginasAppsc Aee Mains 2019 Electrical Engineering Paper III 1fcbb2c9SURYA PRAKASHAinda não há avaliações
- Project Report On HeritageDocumento39 páginasProject Report On HeritageBALA YOGESH YANDAMURIAinda não há avaliações
- The Story of An Hour QuestionpoolDocumento5 páginasThe Story of An Hour QuestionpoolAKM pro player 2019Ainda não há avaliações
- How Do I Predict Event Timing Saturn Nakshatra PDFDocumento5 páginasHow Do I Predict Event Timing Saturn Nakshatra PDFpiyushAinda não há avaliações
- Using MonteCarlo Simulation To Mitigate The Risk of Project Cost OverrunsDocumento8 páginasUsing MonteCarlo Simulation To Mitigate The Risk of Project Cost OverrunsJancarlo Mendoza MartínezAinda não há avaliações
- Review On Antibiotic Reidues in Animl ProductsDocumento6 páginasReview On Antibiotic Reidues in Animl ProductsMa. Princess LumainAinda não há avaliações
- Color Coding Chart - AHGDocumento3 páginasColor Coding Chart - AHGahmedAinda não há avaliações
- GSP AllDocumento8 páginasGSP AllAleksandar DjordjevicAinda não há avaliações
- Market Structure and TrendDocumento10 páginasMarket Structure and TrendbillAinda não há avaliações
- (LaSalle Initiative) 0Documento4 páginas(LaSalle Initiative) 0Ann DwyerAinda não há avaliações
- B1 Editable End-of-Year TestDocumento6 páginasB1 Editable End-of-Year TestSyahira Mayadi50% (2)
- Promotion of Coconut in The Production of YoghurtDocumento4 páginasPromotion of Coconut in The Production of YoghurtԱբրենիկա ՖերլինAinda não há avaliações
- Security Policy 6 E CommerceDocumento6 páginasSecurity Policy 6 E CommerceShikha MehtaAinda não há avaliações
- Quality Assurance Plan-75FDocumento3 páginasQuality Assurance Plan-75Fmohamad chaudhariAinda não há avaliações
- By Vaibhav Pandya S R.information Security Consultant M.Tech Solutions (India) PVT - LTDDocumento22 páginasBy Vaibhav Pandya S R.information Security Consultant M.Tech Solutions (India) PVT - LTDtsegay.csAinda não há avaliações
- Cognitive Coaching AdelaideDocumento3 páginasCognitive Coaching AdelaideBusiness-Edu100% (2)
- Pharmacy System Project PlanDocumento8 páginasPharmacy System Project PlankkumarAinda não há avaliações
- All About History History of Communism - 4th Edition 2022Documento148 páginasAll About History History of Communism - 4th Edition 2022Duke100% (1)
- Self-Efficacy and Academic Stressors in University StudentsDocumento9 páginasSelf-Efficacy and Academic Stressors in University StudentskskkakleirAinda não há avaliações
- July 2014Documento56 páginasJuly 2014Gas, Oil & Mining Contractor MagazineAinda não há avaliações
- Mars Atlas MOM 8 13Documento6 páginasMars Atlas MOM 8 13aldert_pathAinda não há avaliações
- Body Temperature PDFDocumento56 páginasBody Temperature PDFBanupriya-Ainda não há avaliações
- YS1700 Drum Level ControlDocumento2 páginasYS1700 Drum Level ControlIdriss BarçaAinda não há avaliações
- Description About Moon: Earth SatelliteDocumento6 páginasDescription About Moon: Earth SatellitePurva KhatriAinda não há avaliações
- Quality Assurance Plan - CivilDocumento11 páginasQuality Assurance Plan - CivilDeviPrasadNathAinda não há avaliações
- Invenio Flyer enDocumento2 páginasInvenio Flyer enErcx Hijo de AlgoAinda não há avaliações
- ACTIVITY Design - Nutrition MonthDocumento7 páginasACTIVITY Design - Nutrition MonthMaria Danica89% (9)
- Catalog de Aparatura Si Instrumentar Veterinar Eikemeyer-GermaniaDocumento336 páginasCatalog de Aparatura Si Instrumentar Veterinar Eikemeyer-GermaniaDr. Dragos CobzariuAinda não há avaliações
- Supreme Court Case Analysis-Team ProjectDocumento5 páginasSupreme Court Case Analysis-Team ProjectJasmineA.RomeroAinda não há avaliações