Você também pode gostar
- Peripheral Nerve InjuriesDocumento29 páginasPeripheral Nerve InjuriesbrillniksAinda não há avaliações
- Peripheral Nerve LesionDocumento11 páginasPeripheral Nerve LesionBalaKrishnaAinda não há avaliações
- Nerve InjuriesDocumento20 páginasNerve InjuriesAnupama NagrajAinda não há avaliações
- Multiple Sclerosis: Practical Comprehensive EssentialsNo EverandMultiple Sclerosis: Practical Comprehensive EssentialsAinda não há avaliações
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsAinda não há avaliações
- FR Distal HumerusDocumento55 páginasFR Distal Humerusiisscribd100% (1)
- Femoral Neck FracturesDocumento8 páginasFemoral Neck FracturesMorshed Mahbub AbirAinda não há avaliações
- Radial NerveDocumento47 páginasRadial NerveFadilla PermataAinda não há avaliações
- Trauma & Orthopaedic SurgeryDocumento120 páginasTrauma & Orthopaedic SurgeryOstazAinda não há avaliações
- Clinical Examination of Hip JointDocumento71 páginasClinical Examination of Hip JointDeevi Mohana SasankAinda não há avaliações
- Radial Forearm Free FlapDocumento54 páginasRadial Forearm Free FlapWakilAhmadAinda não há avaliações
- 12 - Fractures & Dislocations of The Upper Limb-1Documento84 páginas12 - Fractures & Dislocations of The Upper Limb-1Ain Ul NoorAinda não há avaliações
- Patellar FractureDocumento25 páginasPatellar FractureSyafiq ShahbudinAinda não há avaliações
- Brachial Plexus InjuriesDocumento64 páginasBrachial Plexus Injuriesprashanth naikAinda não há avaliações
- Upper Extremity FracturesDocumento80 páginasUpper Extremity FracturesSidan EmozieAinda não há avaliações
- Peripheral NerveDocumento6 páginasPeripheral NerveNur Atiqah ZainalAinda não há avaliações
- Perthes Disease: Mohamed Hamood MohamedDocumento4 páginasPerthes Disease: Mohamed Hamood MohamedMohamed HamoodAinda não há avaliações
- Tuberculosis of Hip JointDocumento25 páginasTuberculosis of Hip JointYousra ShaikhAinda não há avaliações
- Bones and Joints TBDocumento19 páginasBones and Joints TBmichaelcylAinda não há avaliações
- Median NerveDocumento40 páginasMedian Nervehumera100% (2)
- Orthopedic: Dislocations of The Hip JointDocumento16 páginasOrthopedic: Dislocations of The Hip JointAnmarAinda não há avaliações
- Compressive Neuropathy of Upper LimbDocumento49 páginasCompressive Neuropathy of Upper LimbYamunaVaaneeSivalingamAinda não há avaliações
- Claw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandClaw Hand, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNota: 4 de 5 estrelas4/5 (1)
- Table of Upper Limb MusclesDocumento4 páginasTable of Upper Limb MusclessuperdobbyAinda não há avaliações
- An Insider's Guide to Orthopedic Surgery: A Physical Therapist Shares the Keys to a Better RecoveryNo EverandAn Insider's Guide to Orthopedic Surgery: A Physical Therapist Shares the Keys to a Better RecoveryNota: 4 de 5 estrelas4/5 (1)
- Peripheral Nerve Examination (Final)Documento2 páginasPeripheral Nerve Examination (Final)Nurul Amalina OsmanAinda não há avaliações
- Shortcut to Orthopaedics: What's Common and What's Important for Canadian Students and Primary Care PhysiciansNo EverandShortcut to Orthopaedics: What's Common and What's Important for Canadian Students and Primary Care PhysiciansAinda não há avaliações
- Anatomy of HandDocumento54 páginasAnatomy of Handromaisa akhtar100% (1)
- Peripheral Nerve InjuriesDocumento25 páginasPeripheral Nerve InjuriesaboujisAinda não há avaliações
- 3.5 MM LCP Anterolateral Distal de TibiaDocumento27 páginas3.5 MM LCP Anterolateral Distal de TibiaAlfredo AlfredoAinda não há avaliações
- Elbow Joint CHP 10 PDFDocumento42 páginasElbow Joint CHP 10 PDFAlfionita WikaAinda não há avaliações
- Avascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandAvascular Necrosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNota: 4 de 5 estrelas4/5 (2)
- Rehabilitation of Adults With Upper-Limb AmputationsDocumento59 páginasRehabilitation of Adults With Upper-Limb AmputationsSameeha AbbassAinda não há avaliações
- Current Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderNo EverandCurrent Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderAinda não há avaliações
- Principles and Management of Acute Orthopaedic Trauma: Third EditionNo EverandPrinciples and Management of Acute Orthopaedic Trauma: Third EditionAinda não há avaliações
- Tendon Injuries of Hand: DR Saumya AgarwalDocumento101 páginasTendon Injuries of Hand: DR Saumya AgarwaltesfahuntekletilahunAinda não há avaliações
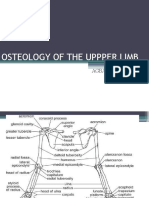
- Osteology of Upper LimbDocumento63 páginasOsteology of Upper LimbAkomolede AbosedeAinda não há avaliações
- Thoracic Outlet Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo EverandThoracic Outlet Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNota: 5 de 5 estrelas5/5 (1)
- Principles of Non Operative Fracture ManagementDocumento29 páginasPrinciples of Non Operative Fracture Managementronny100% (3)
- CTEVDocumento61 páginasCTEVSylvia LoongAinda não há avaliações
- Acetabular Fracture PostgraduateDocumento47 páginasAcetabular Fracture Postgraduatekhalidelsir5100% (1)
- Wrist Complex1Documento25 páginasWrist Complex1bpt2100% (1)
- Tennis ElbowDocumento13 páginasTennis ElbowPadma PadalAinda não há avaliações
- Orthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Documento13 páginasOrthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Tomas Kurakovas100% (1)
- Hand IncisionsDocumento55 páginasHand IncisionsDabessa Mosissa100% (2)
- Special Tests For Elbow and ForearmDocumento3 páginasSpecial Tests For Elbow and ForearmAllyza PenaAinda não há avaliações
- Knee MechanicsDocumento107 páginasKnee MechanicsAhmed El goharyAinda não há avaliações
- UKA: When Would I Do It?Documento35 páginasUKA: When Would I Do It?neareastspineAinda não há avaliações
- Lower LimbDocumento53 páginasLower LimbRupesh M DasAinda não há avaliações
- Erbs PalsyDocumento9 páginasErbs PalsyVatsalVermaAinda não há avaliações
- Ortho Review 1Documento67 páginasOrtho Review 1mark tAinda não há avaliações
- Low Back Exam PDFDocumento2 páginasLow Back Exam PDFDeeea1991Ainda não há avaliações
- Radial Nerve: Rajadurai R Crri, Orthopedics Ii Unit RGGGHDocumento31 páginasRadial Nerve: Rajadurai R Crri, Orthopedics Ii Unit RGGGHrajaeasAinda não há avaliações
- A Brief Introduction Into Orthopaedic ImplantsDocumento20 páginasA Brief Introduction Into Orthopaedic ImplantsLuisAngelPonceTorresAinda não há avaliações
- Osteoarthritis of KneeDocumento34 páginasOsteoarthritis of KneeKOMALAinda não há avaliações
- Orthopedic SurgeryDocumento53 páginasOrthopedic SurgeryGeorgeAinda não há avaliações
- Total Hip Replacement PPDocumento22 páginasTotal Hip Replacement PPAnonymous dGfXuDd5Ainda não há avaliações
- Muscular Dystrophy......Documento30 páginasMuscular Dystrophy......Rupika SodhiAinda não há avaliações
- Pes Cavus ....Documento34 páginasPes Cavus ....Rupika Sodhi100% (2)
- Pressure SoresDocumento20 páginasPressure SoresRupika Sodhi100% (1)
- Accelerated ACL Rehabilitation 2007 - 2Documento32 páginasAccelerated ACL Rehabilitation 2007 - 2Rupika SodhiAinda não há avaliações
- Physiotherapy Management of Tennis Elbow................ ArticleDocumento5 páginasPhysiotherapy Management of Tennis Elbow................ ArticleRupika SodhiAinda não há avaliações
- Stages of Bone Healing After FractureDocumento2 páginasStages of Bone Healing After FractureRamelyn TolentinoAinda não há avaliações
- C-ECN321 MC Questions Ch1-Ch12 ExamplesDocumento2 páginasC-ECN321 MC Questions Ch1-Ch12 ExamplesKevin WroblewskiAinda não há avaliações
- Cpccohs2001a Final Assessment PracticalDocumento29 páginasCpccohs2001a Final Assessment PracticalPriyanka ThakurAinda não há avaliações
- Torts Midterms Reviewer Final PDFDocumento9 páginasTorts Midterms Reviewer Final PDFDarla GreyAinda não há avaliações
- 1920 1924Documento16 páginas1920 1924api-246211793Ainda não há avaliações
- Sexual OffencesDocumento21 páginasSexual Offencesniraj_sdAinda não há avaliações
- Dworkin & Maciariello Injury LawDocumento16 páginasDworkin & Maciariello Injury LawBradley DworkinAinda não há avaliações
- AO Trauma Course - Basic Principles of Fracture Management Syllabus For FacultyDocumento27 páginasAO Trauma Course - Basic Principles of Fracture Management Syllabus For FacultyPablo GerardoAinda não há avaliações
- Eiband Curve LsdynaDocumento28 páginasEiband Curve LsdynaKivanc SengozAinda não há avaliações
- Hirac SampleDocumento12 páginasHirac Sampleyelsa otreblaAinda não há avaliações
- TORT 2 WEEK 11 DefencesDocumento7 páginasTORT 2 WEEK 11 DefencesssAinda não há avaliações
- First AidDocumento48 páginasFirst AidPeter AlexanderAinda não há avaliações
- Radiologic Positioning PrinciplesDocumento20 páginasRadiologic Positioning PrinciplesEugene De PanoAinda não há avaliações
- Cymbals PDFDocumento3 páginasCymbals PDFscooterbobAinda não há avaliações
- Systemic Response To InjuryDocumento45 páginasSystemic Response To InjuryAbdulaziz Al-Akhras100% (1)
- Susan Aikens Vs BBC Worldwide Reality Productions (Life Below Zero)Documento32 páginasSusan Aikens Vs BBC Worldwide Reality Productions (Life Below Zero)Kyle Hopkins100% (1)
- Hazard Register ConstructionDocumento15 páginasHazard Register ConstructionMohd ObaidullahAinda não há avaliações
- Stellate Ganglion Block by Dr. JayDocumento32 páginasStellate Ganglion Block by Dr. JayDr Jay Panchal100% (2)
- User Manual For 12K 18K 24KDocumento48 páginasUser Manual For 12K 18K 24KAriel Calero100% (3)
- Task 2 Meet Personal NeedsDocumento3 páginasTask 2 Meet Personal Needsdev kumarAinda não há avaliações
- 8B - Spondylolysis, SpondylolisthesisDocumento14 páginas8B - Spondylolysis, SpondylolisthesismorlaszloAinda não há avaliações
- Peripheral Nervous System NotesDocumento9 páginasPeripheral Nervous System NotesSaoirseAinda não há avaliações
- Ferret OrthopedicsDocumento27 páginasFerret OrthopedicsTayná P DobnerAinda não há avaliações
- Degenerative Spinal DisordersDocumento47 páginasDegenerative Spinal Disordersasad1912Ainda não há avaliações
- Heat Exposure InjuriesDocumento3 páginasHeat Exposure InjuriesKURIMAONGAinda não há avaliações
- Concussion Review - Lori HurtDocumento5 páginasConcussion Review - Lori HurtBob Cook100% (1)
- Allegany FB PreviewDocumento32 páginasAllegany FB Previewtimesnews0% (1)
- Anatomy Trains OverviewDocumento20 páginasAnatomy Trains OverviewDennis Chiu Mee100% (5)
- Assessment and Management of Unconscious PatientDocumento10 páginasAssessment and Management of Unconscious PatientDebasis SahooAinda não há avaliações