Escolar Documentos
Profissional Documentos
Cultura Documentos
CAH El-Maouche2017
Enviado por
Ambar AlinaTítulo original
Direitos autorais
Formatos disponíveis
Compartilhar este documento
Compartilhar ou incorporar documento
Você considera este documento útil?
Este conteúdo é inapropriado?
Denunciar este documentoDireitos autorais:
Formatos disponíveis
CAH El-Maouche2017
Enviado por
Ambar AlinaDireitos autorais:
Formatos disponíveis
Seminar
A Adrenal hormone synthesis and alternative pathways
CYP11B2
StAR HSD3B2 CYP21A2 Deoxy- Aldosterone
Cholesterol Pregnenolone Progesterone
CYP11A1 (POR) corticosterone Corticosterone
(POR) CYP17A1 (POR) CYP17A1 CYP11B1
HSD3B2 CYP21A2 CYP11B1
17-OH-pregnenolone 17-OH-progesterone 11-Deoxy-
Cortisol
(POR) cortisol
(POR) CYP17A1 (POR) CYP17A1
HSD3B2 SRD5A1
DHEA Androstenedione
CYP11B1 (POR) CYP19A1 HSD17B3
5α-pregnane- AKR1C1/3 17-OH-
11-keto- 11-keto- 11β-OH-
Oestrone Testosterone 7α-ol-3, 20-dione Allopregnanolone
androstanedione androstenedione androstenedione
CYP11B1 (POR) CYP19A1 SRD5A2 (POR) CYP17A1
HSD17B AKR1C1/3
11-keto-DHT 11-keto-T 11β-OH-T Oestradiol DHT Androstanediol Androsterone
B 21-hydroxylase deficiency
CYP11B2
StAR HSD3B2 CYP21A2 Deoxy- Aldosterone
Cholesterol Pregnenolone Progesterone
CYP11A1 corticosterone Corticosterone
CYP17A1 CYP17A1 CYP11B1
HSD3B2 CYP21A2 CYP11B1
17-OH-pregnenolone 17-OH-progesterone 11-Deoxy-
Cortisol
cortisol
CYP17A1 CYP17A1
HSD3B2
DHEA Androstenedione
CYP11B1 CYP19A1 HSD17B3
5α-pregnane- AKR1C1/3 17-OH-
11-keto- 11-keto- 11β-OH-
Oestrone Testosterone 7α-ol-3, 20-dione Allopregnanolone
androstanedione androstenedione androstenedione
CYP11B1 CYP19A1 SRD5A2 (POR) CYP17A1
HSD17B AKR1C1/3
11-keto-DHT 11-keto-T 11β-OH-T Oestradiol DHT Androstanediol Androsterone
C 11β-hydroxylase deficiency
CYP11B2
StAR HSD3B2 CYP21A2 Deoxy- Aldosterone
Cholesterol Pregnenolone Progesterone
CYP11A1 corticosterone Corticosterone
CYP17A1 CYP17A1 CYP11B1
17-OH-pregnenolone HSD3B2 17-OH-progesterone CYP21A2 11-Deoxy- CYP11B1
Cortisol
cortisol
CYP17A1 CYP17A1
HSD3B2
DHEA Androstenedione
CYP19A1 HSD17B3
Oestrone Testosterone
CYP19A1 SRD5A2
Oestradiol DHT
D 17-hydroxylase deficiency
CYP11B2
StAR HSD3B2 CYP21A2 Deoxy- Aldosterone
Cholesterol Pregnenolone Progesterone
CYP11A1 corticosterone Corticosterone
CYP17A1* CYP17A1* CYP11B1
17-OH-pregnenolone HSD3B2 17-OH-progesterone CYP21A2 11-Deoxy- CYP11B1
Cortisol
cortisol
CYP17A1** CYP17A1**
HSD3B2
DHEA Androstenedione
CYP19A1 HSD17B3
Oestrone Testosterone
CYP19A1 SRD5A2
Oestradiol DHT
(Figure 2 continues on next page)
2196 www.thelancet.com Vol 390 November 11, 2017
Seminar
E 3β–hydroxysteroid dehydrogenase type 2 deficiency
CYP11B2
StAR HSD3B2 CYP21A2 Deoxy- Aldosterone
Cholesterol Pregnenolone Progesterone
CYP11A1 corticosterone Corticosterone
CYP17A1 CYP17A1 CYP11B1
17-OH-pregnenolone HSD3B2 17-OH-progesterone CYP21A2 11-Deoxy- CYP11B1
Cortisol
cortisol
CYP17A1 CYP17A1
HSD3B2
DHEA Androstenedione
CYP19A1 HSD17B3
Oestrone Testosterone
CYP19A1 SRD5A2
Oestradiol DHT
F P450 oxidoreductase deficiency
CYP11B2
StAR HSD3B2 CYP21A2 Deoxy- Aldosterone
Cholesterol Pregnenolone Progesterone
CYP11A1 POR corticosterone Corticosterone
POR CYP17A1 POR CYP17A1 CYP11B1
HSD3B2 CYP21A2 11-Deoxy- CYP11B1
17-OH-pregnenolone 17-OH-progesterone Cortisol
POR cortisol
POR CYP17A1 POR CYP17A1
HSD3B2
DHEA Androstenedione
POR CYP19A1 HSD17B3
5α-pregnane- AKR1C1/3 17-OH-
Oestrone Testosterone 7α-ol-3, 20-dione Allopregnanolone
POR CYP19A1 SRD5A2 (POR) CYP17A1
HSD17B AKR1C1/3
Oestradiol DHT Androstanediol Androsterone
G Lipoid congenital adrenal hyperplasia or P450 cholesterol side chain cleavage
CYP11B2
StAR HSD3B2 CYP21A2 Deoxy- Aldosterone
Cholesterol Pregnenolone Progesterone
CYP11A1 corticosterone Corticosterone
CYP17A1 CYP17A1 CYP11B1
HSD3B2 CYP21A2 11-Deoxy- CYP11B1
17-OH-pregnenolone 17-OH-progesterone Cortisol
cortisol
CYP17A1 CYP17A1
HSD3B2
DHEA Androstenedione
CYP19A1 HSD17B3
Oestrone Testosterone
CYP19A1 SRD5A2
Oestradiol DHT
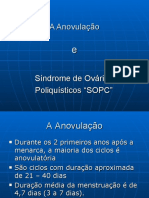
Figure 2: Adrenal steroidogenesis pathways
(A) Classic steroidogenesis pathway and alternative pathways leading to androgen production in the light yellow boxes. (B) 21-hydroxylase deficiency, (C)
11β-hydroxylase deficiency, (D) 17-hydroxylase deficiency, (E) 3β-hydroxysteroid dehydrogenase type 2 deficiency, (F) P450 oxidoreductase deficiency, and (G) lipoid
congenital adrenal hyperplasia and P450 cholesterol side chain cleavage deficiency, with impact of specific impairments on the adrenal steroidogenic pathway. Genes
in which mutations cause congenital adrenal hyperplasia are shown in red. Light grey denotes deficient hormones at low concentrations due to the preceding block in
steroid production. Dashed arrows denote indirect suppression of the subsequent hormone. Dashed lines across enzymes denote apparent enzyme deficiency.
DHEA=dehydroepiandrosterone. DHT=5α-dihydrotestosterone. T=testosterone. POR=P450 oxidoreductase.
renin–angiotensin system suppression might not occur 17OH deficiency
in the neonatal period because of renal mineralocorticoid The CYP17A1 gene encodes an enzyme that expresses both
resistance that is present in the first few months of life. 17α-hydroxylase and 17,20-lyase activities (table 1). Because
Clinically, patients with 11βOH deficiency present of the location of the enzyme in the steroidogenic pathway,
similarly to patients with 21OH deficiency with signs of severe mutations in the gene impair adrenal and gonadal
androgen excess, but patients with 11βOH also have sex steroid production (figure 2), which causes sexual
hypertension rather than salt loss (table 2).32 A non- infantilism and puberty failure (table 2).35 Production of
classic form of enzyme deficiency caused by CYP11B1 dehydroepiandrosterone is blocked, which prevents
mutations exists but is very rare.45 adrenarche and development of pubic and axillary hair.
www.thelancet.com Vol 390 November 11, 2017 2197
Seminar
21-hydroxylase 11β-hydroxylase 17α-hydroxylase/ 3β-hydroxy-steroid P450 oxidoreductase Lipoid adrenal Cholesterol side
deficiency deficiency 17,20-lyase deficiency dehydrogenase deficiency hyperplasia chain cleavage
type 2 deficiency enzyme deficiency
Affected gene CYP21A2 (201910) CYP11B1 (202010) CYP17A1 (202110) HSD3B2 (201810) POR (201750) StAR (600617) CYP11A1 (118485)
(OMIM number)
Incidence Classic: 1:10 000 to 1:100 00032 in Caucasians, 1:50 00034
Rare Rare, 130 cases from Rare, mostly Rare, <30 patients,
1:20 00025 1:600033 in Moroccan Increased frequency in 11 countries reported36 Japanese, Korean, mostly from eastern
Non-classic: 1:20027 Jews* Brazil*34,35 and Palestinian Turkey38
to 1:100026 Non-classic: unknown populations 37
Affected organs Adrenal glands Adrenal glands Adrenal glands and Adrenal glands and Adrenal glands, gonads, Adrenal glands and Adrenal glands and
gonads gonads liver, and skeletal gonads gonads
Disorder of sex Classic: 46,XX Classic: 46,XX 46,XY Classic: 46,XY, 46,XX 46,XX, 46,XY 46,XY 46,XY
development Non-classic: No Non-classic: No (rare) (variable) Non-classic: 46,XY Non-classic: 46,XY
Non-classic: No (variable) (variable)
Salt wasting Classic: Yes No No Yes No Classic: yes Classic: Yes
Non-classic: No Non-classic: minimal Non-classic: minimal
to none to none
Hypertension No Yes Yes No Yes No No
Non-classic: variable
Postnatal Classic: yes Classic: Yes No Classic: 46,XX No No No
virilisation Non-classic: yes Non-classic: Yes Non-classic: 46,XX
Sex steroid No No Yes Classic: Yes Yes Yes Yes
deficiency Non-classic: No Non-classic: variable Non-classic: variable
Other ·· ·· ·· ·· With or without skeletal ·· ··
malformations
With or without
maternal virilisation
OMIM=Online Mendelian Inheritance in Man. POR=P450 oxidoreductase. StAR= steroidogenic acute regulatory protein. *Due to presence of a founder mutation.
Table 1: Genetic causes and clinical features of the various forms of congenital adrenal hyperplasia
CYP17A1 is expressed in the adrenal zona fasciculata and Impaired 3βHSD2 functionality results in de
zona reticularis but not in the zona glomerulosa. Therefore, creased concentrations of aldosterone, cortisol, and
ACTH-mediated steroidogenesis results in elevated androstenedione, with a subsequent increase in the
concentrations of deoxycorticosterone and corticosterone. concentrations of renin, ACTH, and dehydro
High concentrations of deoxycorticosterone cause epiandrosterone (figure 2). Dehydro epiandrosterone
sodium retention, hypertension, and hypokalaemia, with can be converted to testosterone by extra-adrenal
suppression of aldosterone production. The presence of 3βHSD1. Patients present in infancy with a salt-wasting
corticosterone, which has glucocorticoid activity, prevents adrenal crisis, underdeveloped 46,XY genitalia, and
patients from having an adrenal crisis, even though rarely 46,XX virilisation (table 2).48
cortisol production is low or absent. Both 46,XX and 46,XY The hormonal criteria for diagnosis of 3βHSD2
patients with 17OH deficiency have female external deficiency have changed over the past three decades
genitalia and usually present during puberty as girls because the initial studies identifying a possible non-
without secondary sexual characteristics, with hyper classic form were not based on genetic findings and
gonadotropic hypogonadism, and low-renin hypertension subsequent genetic studies failed to confirm the
(table 2). Isolated 17,20-lyase-deficiency has been reported46 diagnosis.49–51 Non-classic 3βHSD2 deficiency exists, but
but is extremely rare and in truly isolated forms is caused is extremely rare.
by mutations in cytochrome b5, the co-factor needed by
CYP17A1 to exert 17,20 lyase activity.47 Although phenotype POR deficiency
variability occurs, a non-classic form with subtle clinical POR plays a key role in electron transport in the
manifestations has not been defined. endoplasmic reticulum, and several enzymes including
17OH, 21OH, and aromatase depend on POR for their
3βHSD2 deficiency catalytic activity (figure 2). The discovery of POR
3β-hydroxysteroid dehydrogenase exists in two isoforms, deficiency, in 2004,16,17 provided an explanation for
type 1 (3βHSD1) and type 2 (3βHSD2), which are encoded multiple hormonal deficiency, initially known as
by HSD3B1 and HSD3B2 genes, respectively (table 1). apparent combined 17OH and 21OH deficiency.
The HSD3B2 gene is highly expressed in the adrenals Insufficient placental aromatisation of fetal androgens
and gonads, while HSD3B1 is expressed in the placenta could contribute to the virilisation seen in some mothers
and peripheral tissues. carrying babies affected by POR deficiency. However, the
2198 www.thelancet.com Vol 390 November 11, 2017
Seminar
Clinical presentation Hormonal profile Cosyntropin stimulation testing* Other testing
21-hydroxylase Classic: atypical genitalia (46,XX), ↑ 17OHP, 21-deoxycortisol, androstenedione, 17OHP >30 nmol/L (>1000 ng/dL) Non-classic: early morning
deficiency neonatal salt wasting (75%), and and renin (several times higher for classic) follicular phase 17OHP<6 nmol/L
virilisation <4 year old (46,XY) ↓ Cortisol and aldosterone (<200 ng/dL) usually excludes
Non-classic: precocious pubarche, non-classic congenital adrenal
hirsutism, oligomenorrhea/amenorrhea, hyperplasia
and female infertility
11β-hydroxylase Classic: atypical genitalia (46,XX), ↑ DOC, 11-deoxycortisol, androstenedione 11-deoxycortisol >3 times the upper ··
deficiency virilisation <4 years old (46,XY), and 17OHP (mild) limit of normal (several times higher
hypertension, and hypokalaemia ↓ Cortisol, aldosterone, corticosterone, and for classic)
Non-classic: precocious pubarche, renin
hirsutism, oligomenorrhea/amenorrhea,
female infertility, and with or without
hypertension
17α-hydroxylase/ Adolescent female with absence of ↑ DOC, corticosterone (>115 nmol/L, Poor response of ··
17,20-lyase deficiency secondary sexual characteristics, 4000 ng/dL), and progesterone 17-hydroxypregnenolone and 17OHP
hypertension, and hypokalaemia ↓ Cortisol, aldosterone, Elevated ratios of DOC to cortisol and
17-hydroxypregnenolone, 17OHP, renin, corticosterone to sex steroids
DHEA, and androstenedione
3β-hydroxysteroid Atypical genitalia (46,XX: rare, mild; ↑ 17-hydroxypregnenolone, DHEA, and renin 17-hydroxypregnenolone Poor testosterone response hCG
dehydrogenase type 2 46,XY), neonatal salt wasting ↓ Cortisol, aldosterone, progesterone, 17OHP, >150 nmol/L (5000 ng/dL) stimulation in infancy
deficiency Non-classic: precocious pubarche, androstenedione, DOC, and 11-deoxycortisol Elevated ratios pregnenolone to
hirsutism, and oligomenorrhea/ progesterone and
amenorrhea (46,XX); atypical genitalia 17-hydroxypregnenolone to 17OHP
(46,XY; mild)
P450 oxidoreductase Atypical genitalia, with or without ↑ Pregnenolone, progesterone, 17OHP, DOC, Variable 17OHP response, variable Urine steroid metabolite profile
deficiency skeletal manifestation (Antley-Bixler), and corticosterone cortisol response (often inadequate) shows characteristic diagnostic
and with or without maternal virilisation ↓ DHEA and androstenedione profile
Variable (normal or low): cortisol, aldosterone
Lipoid adrenal Classic: female genitalia, neonatal ↑ Renin Minimal to no response Classic: minimal response hCG
hyperplasia or SCC salt wasting ↓ All steroids Non-classic: variable response, stimulation
enzyme deficiency Non-classic: adrenal insufficiency (2 years Non-classic: variable ↓cortisol common Genetic testing needed to
to adulthood), variable gonadal differentiate lipoid congenital
function, variable genitalia (46,XY: mild) adrenal hyperplasia and SCC
deficiency
17OHP=17-hydroxyprogesterone. DHEA=dehydroepiandrosterone. DOC=deoxycorticosterone. hCG=human chorionic gonadotropin. SCC=side chain cleavage. *Administration of standard dose of 250 µg
cosyntropin (in very low birthweight infants the dose may be reduced to 0·125 µg), concomitant measurement of 17OHP, cortisol, DOC, 11-DOC, 17-hydroxypregnenelone, DHEA, and androstenedione at
baseline and 60 min to distinguish 21-hydroxylase deficiency from other rarer forms of congenital adrenal hyperplasia.
Table 2: Clinical presentation and biochemical findings
production of androgens via an alternative pathway to radiohumeral synostosis, midface hypoplasia, and other
the one that produces the most potent androgen, non- skeletal manifestations that resemble the Antley-Bixler
aromatisable 5-dihydrotestosterone, might also explain syndrome can occur.16
the prenatal virilisation of female patients affected by Generally, patients with POR deficiency do not have
POR deficiency, while affected individuals have postnatal mineralocorticoid deficiency as impairment of
sex steroid deficiency.17 POR also acts as an electron 17α-hydroxylase increases production of mineral
donor to cytochrome P450 (CYP) enzymes other than ocorticoid intermediates, and affected adults can
steroidogenic CYP enzymes, which explains POR develop hypertension.16,36 Patients have variable cortisol
deficiency-associated changes in drug metabolism52 and responses to cosyntropin testing, with most patients
the pathogenesis of skeletal dysplasia, which is often requiring either permanent or stress dose glucocorticoid
seen in patients.53 coverage.36
Most POR mutations retain some enzymatic function;
homozygous mutations with complete loss of function Lipoid congenital adrenal hyperplasia
might not be viable, as seen in rodent models.54 Classic lipoid congenital adrenal hyperplasia is
Presentation of patients with POR mutations varies from characterised by deficiency of all steroid hormones and
mildly affected women with amenorrhea and polycystic is due to StAR mutations (table 1, figure 2). StAR
ovaries or men with androgen deficiency, to severe regulates the transfer of cholesterol from the outer to
hormone disturbances causing atypical genitalia in both inner mitochondrial membrane, a key step in the
46,XX and 46,XY patients (table 1, 2). 46,XX virilisation initiation of steroidogenesis. When cholesterol cannot
does not progress, and patients postnatally have sex be mobilised, adrenal lipid droplets accumulate and are
steroid deficiency. Craniosynostosis, radioulnar or seen on autopsy, hence the name lipoid congenital
www.thelancet.com Vol 390 November 11, 2017 2199
Você também pode gostar
- Fitoterápicos para LibidoDocumento6 páginasFitoterápicos para LibidoSolange FernandesAinda não há avaliações
- 12 - Aparelho Reprodutor Masculino - MedresumosDocumento4 páginas12 - Aparelho Reprodutor Masculino - MedresumosaeadaAinda não há avaliações
- Aula 2 Metabolismo OsteomineralDocumento29 páginasAula 2 Metabolismo OsteomineralDayane Costa De SouzaAinda não há avaliações
- Reprodução HumanaDocumento40 páginasReprodução HumanaLeonardo GenesioAinda não há avaliações
- FICHA DE INSCRIÇÃO Hidro NovaDocumento3 páginasFICHA DE INSCRIÇÃO Hidro NovaSuelly Eduarda EseAinda não há avaliações
- Biologia Exercicios Fisiologia Animal Sistema Endocrino Gabarito ResolucaoDocumento18 páginasBiologia Exercicios Fisiologia Animal Sistema Endocrino Gabarito ResolucaoIsadora Melo FrancoAinda não há avaliações
- A Anovulação e PCODocumento36 páginasA Anovulação e PCOEliotélioMirandaNhamicoleAinda não há avaliações
- Ficha de Anamnese FacialDocumento2 páginasFicha de Anamnese FacialGil A. PalacioAinda não há avaliações
- Ficha Formativa N 1 - 12 BioDocumento8 páginasFicha Formativa N 1 - 12 BioGlennda Jorge PinheiroAinda não há avaliações
- Diabetes M Manual PTDocumento12 páginasDiabetes M Manual PTSofia PinheiroAinda não há avaliações
- RelatorioDocumento14 páginasRelatorioFilipa100% (1)
- Biologia - 12º Ano oDocumento24 páginasBiologia - 12º Ano oMiguel100% (1)
- GINECOLOGIA e OBSTETRIěCIA PDFDocumento34 páginasGINECOLOGIA e OBSTETRIěCIA PDFKetoly Pascoal ColatiAinda não há avaliações
- Parto EutócicoDocumento9 páginasParto EutócicoAlessandra DiasAinda não há avaliações
- Hormônios Sexuais e Métodos ContraceptivosDocumento13 páginasHormônios Sexuais e Métodos ContraceptivosDêh Andrade100% (1)
- Cap. 14 - Sistema EndocrinoDocumento7 páginasCap. 14 - Sistema EndocrinoSuzane LobatoAinda não há avaliações
- Sistema HormonalDocumento22 páginasSistema HormonalJoão GomesAinda não há avaliações
- PuberdadeDocumento18 páginasPuberdadeEvandra CustódioAinda não há avaliações
- Sistema Reprodutor Lista Biologia Prof LuanDocumento4 páginasSistema Reprodutor Lista Biologia Prof LuanJonathasAinda não há avaliações
- Maneio Cadela PDFDocumento62 páginasManeio Cadela PDFÉrica TeixeiraAinda não há avaliações
- Sistema EndocrinoDocumento11 páginasSistema EndocrinoPaola BTAinda não há avaliações
- Tipos de Hormônios TransfemininosDocumento2 páginasTipos de Hormônios TransfemininosalineAinda não há avaliações
- Ndulostireoidianos 200512 144651 1589379250Documento38 páginasNdulostireoidianos 200512 144651 1589379250RICARDO DE ASSIS DUTRA SANTOSAinda não há avaliações
- Trabalho de Biologia Coordenação HormonalDocumento16 páginasTrabalho de Biologia Coordenação HormonalBráulioAinda não há avaliações
- Gametogenese OogeneseDocumento52 páginasGametogenese OogeneseGabriel Henrique LopesAinda não há avaliações
- Sistema ReprodutorDocumento25 páginasSistema ReprodutorAngela TeixeiraAinda não há avaliações
- Capítulo 81 - Fisiologia Feminina Antes Da Gravidez e Hormônios Femininos - 4 PáginasDocumento4 páginasCapítulo 81 - Fisiologia Feminina Antes Da Gravidez e Hormônios Femininos - 4 PáginasandreamokadaAinda não há avaliações
- Diabetes e Gestao Diagnstico e ComplicaesDocumento42 páginasDiabetes e Gestao Diagnstico e Complicaesnatanael sousaAinda não há avaliações
- Biologia: Sistema Endócrino e Sua FisiologiaDocumento5 páginasBiologia: Sistema Endócrino e Sua FisiologiaJack da casa que jack ConstruíuAinda não há avaliações
- 517-Regulação Hormonal No Metabolismo Energetico de Não Ruminantes Texto Do Artigo-2354-1-11-20210228Documento14 páginas517-Regulação Hormonal No Metabolismo Energetico de Não Ruminantes Texto Do Artigo-2354-1-11-20210228Chirley RibeiroAinda não há avaliações