Escolar Documentos
Profissional Documentos
Cultura Documentos
02 (06) Final Cistos CPA
Enviado por
kallanpulio10_2550 notas0% acharam este documento útil (0 voto)
13 visualizações6 páginasDireitos autorais
© © All Rights Reserved
Formatos disponíveis
PDF, TXT ou leia online no Scribd
Compartilhar este documento
Compartilhar ou incorporar documento
Você considera este documento útil?
Este conteúdo é inapropriado?
Denunciar este documentoDireitos autorais:
© All Rights Reserved
Formatos disponíveis
Baixe no formato PDF, TXT ou leia online no Scribd
0 notas0% acharam este documento útil (0 voto)
13 visualizações6 páginas02 (06) Final Cistos CPA
Enviado por
kallanpulio10_255Direitos autorais:
© All Rights Reserved
Formatos disponíveis
Baixe no formato PDF, TXT ou leia online no Scribd
Você está na página 1de 6
Reviso
J Bras Neurocirurg 22 (3): 66-71, 2011
Mattei TA, Goulart CR, Lima JS, Ramina R - Differential Diagnosis and Surgical Management of Cerebellopontine Angle Cystic Lesions
66
Differential Diagnosis and Surgical Management
of Cerebellopontine Angle Cystic Lesions
Tobias Alcio Mattei, M.D.
1
Carlos R. Goulart, B.S
2
Julia Schemes de Lima, B.S.
3
Ricardo Ramina, M.D, PhD.
4
1. Neurosurgery Department University of Illinois at Peoria IL/USA
2. President of League of Neurosurgery of Instituto de Neurologia de Curitiba Brazil
3. Medical Illustrator - League of Neurosurgery Instituto de Neurologia de Curitiba Brazil
4. Chief of Neurosurgery Department of Instituto de Neurologia de Curitiba Brazil
SUMRIO
A maioria dos tumores de ngulo ponto-cerebelar em adultos
so benignos e extra-axiais. A leso mais comum do ngulo
ponto-cerebelar (schwannoma vestibular) familiar maioria
dos neurocirurgies. Entretanto leses csticas do ngulo
ponto-cerebelar merecem uma anlise cuidadosa, levando-se
em considerao uma ampla gama de diagnsticos diferenciais,
dentre os quais: cistos epidermides, cistos aracnides,
neurinomas csticos, meningiomas csticos, bem como outras
entidades mais raras como leses vasculares e tumorais
malignas. Os autores apresentam uma reviso critica da
literatura, proporcionando ao leitor uma viso geral sobre os
possveis diagnsticos diferenciais bem como atuais diretrizes
para a avaliao imagenolgica de leses csticas no ngulo
ponto-cerebelar.
Palavras-chave: ngulo ponto-cerebelar, cisto epidermide,
cisto aracnide, neurinoma do acstico, schwannoma
vestibular, diagnstico diferencial, tratamento cirrgico.
ABSTRACT
Cerebellopontine angle (CPA) tumors in adults are mainly
benign and extra-axial. Although the most common CPA lesion
(vestibular schwannoma) is familiar to most neurosurgeons,
cystic lesions of the CPA do pose an important diagnostic
challenge demanding a careful consideration of a wide
range of differential diagnosis including: epidermoid cysts,
arachnoid cysts, cystic schwannomas, cystic meningiomas
as well as other rare entities such as vascular and malignant
tumoral lesions. The authors present a critical review of
the current literature on cystic CPA lesions, providing an
overview about possible differentials as well as guidelines for
preoperative imaging evaluation of a cystic CPA lesion.
Keywords: Cerebello-pontine angle, epidermoid cysts,
arachnoid cysts, cystic schwannomas, cystic meningiomas,
diferencial diagnosis, surgical management.
Recebido em 1 de junho de 2011, aceito em 29 de julho de 2011
Reviso
J Bras Neurocirurg 22 (3): 66-71, 2011
Mattei TA, Goulart CR, Lima JS, Ramina R - Differential Diagnosis and Surgical Management of Cerebellopontine Angle Cystic Lesions
67
INTRODUCTION
Cerebellopontine angle tumors in adults are mainly benign
and extra-axial. Cystic lesions of the CPA often pose as an im-
portant challenge to neurosurgeons, demanding a careful pre-
operative evaluation about a wide range of possible differential
diagnosis, as well as a tailored surgical technique according to
each particular lesion.
The possible histopathological diagnosis for a cystic lesion in
the CPA is, in order of frequency: epidermoid cyst, arachnoid
cyst, cystic schwannoma, cystic meningioma and other rare en-
tities, described in few case reports, such as neurocysticercosis,
neurenteric cyst, cavernous malformations as well as malig-
nant tumoral lesions, which may present as cystic heteroge-
neous masses due to intra-tumoral necrosis.
EPIDERMOID CYSTS
Typically epidermoid cists are extra-axial lesions with the ima-
ging signal similar to the cerebrospinal fluid. These tumors
usually show ondulating margins, modeling their shape to ma-
tch with the CPA and insinuating themselves around the ner-
ves and blood vessels in the CPA. A lamellated or onion-skin
appearance and small peripheral rim of calcification may be
seen in few cases.
11
Magnetic resonance imaging (MRI) usually show no enhance-
ment with gadolinium: they are of hipo or iso-intense sign in
T1 weighted (T1W) images with iso or high signal intensity on
T2W images and FLAIR (Fig. 1).
33,34
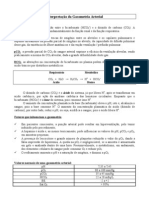
Figure 1. In epidermoid cysts, although MRI sequences may demonstrate an ex-
pansive lesion with compression of the cerebellar parenchyma (Patient 1 -A, B and
C), the lesion usually spread diffusely through the cisternal spaces. (Patient 2 - D,
E and F). These lesions usually are non-enhancing (A and B) and present hype or
isointense signal in T2 (C) and FLAIR (D) and a typical pattern of marked restriction
in diffusion-weighted sequences (E) with typical low apparent diffusion coefficient
(ADC) values (F).
However, the most striking characteristic, which is very sug-
gestive of epidermoid tumors, is the marked restriction (pre-
senting a bright appearance) at Diffusion-weighted imaging
(DWI). The apparent diffusion coefficient (ADC) values of
epidermoid tumors are significantly lower than that of CSF,
and higher than that of deep white matter.
9
There are, however
reports of unusual image findings in epidermoid tumors such
as hyperdensity in computed tomography (CT) and on T1- and
T2-weighted MRI. These late imaging characteristics are thou-
ght to be caused by a high protein concentration within the
content of the cyst.
26
Figure 2. Surgical illustration of a right retrosigmoid approach and intraoperati-
ve images demonstrating surgical ressection of a cystic lesion of the CPA . Note
the white (pearl-like) and non-vascular appearance of the lesion, typical of epider-
moidcysts. (Cr: cranial; Ca: Caudal; Lat: lateral; Med: medial).
Reviso
J Bras Neurocirurg 22 (3): 66-71, 2011
Mattei TA, Goulart CR, Lima JS, Ramina R - Differential Diagnosis and Surgical Management of Cerebellopontine Angle Cystic Lesions
68
Surgery is the only definitive treatment for epidermoid cysts.
However, the decision to operate should be carefully discussed
for each patient, particularly if the patient is asymptomatic.
31
The extent of the lesion at the anterior aspect of the brainstem,
and sometimes above the tentorium, the fragile cortex and ves-
sels, and the hazards of postoperative chemical meningitis often
make such surgery more challenging. Therefore, in many cases,
radical total resection should not be attempted, because the cyst
membrane may be very adherent to local structures such as cra-
nial nerves and surrounding skull base vessels (Fig. 2).
CYSTIC SCHWANNOMAS
Cystic schwannomas are usually larger and present a shorter
time to diagnosis as well as when compared with solid schwan-
nomas. CT scan usually shows a thin rim-enhancement of the
cyst wall. Cystic schwannomas tend to have a funnel-shaped
appearance in the axial MRI and short-club-shaped configu-
ration on the coronal images.
22
There is strong homogeneous
contrast enhancement of the solid components in approximate-
ly half of the tumors.
16,18
Cystic schwannomas can be classified
into three groups: type A - large single cysts with a thin tumor
wall (the most common presentation); type B - single cysts
with a thick tumor wall; type C multi-cystic tumors (Fig. 3).
17
Figure 3. MRI sequences and 3D-reconstruction of a large (3,6 x 2,0 x 2,3 cm)
multi-cystic CPA lesion. The pathological specimen confirmed a vestibular schwan-
noma with areas of cystic degeneration and necrosis.
The cystic components of vestibular schwannomas are well-
correlated with their histological features. Histopathological
analysis of the cyst wall reveals the presence of numerous ab-
normal sinusoid and telangiectasia-like vessels, which may
occasionally reveal signs of thrombosis.
25
The vessel walls
display endothelial proliferation and are frequently hyalinized.
Hemosiderin deposits and hemosiderin-containing phagocytes
are also found near these vessels. Myxoid degeneration and ne-
crosis are evident in vast areas. In fact, such degenerative chan-
ges appear to be the main cause of formation of the large cysts.
As some series suggest, the surgical outcome of cystic vestibu-
lar schwannomas tends to be poorer compared with non-cystic
vestibular schwannomas of matching size.
6,20
There is also evi-
dence that schwannomas may suffer cystic enlargement after
undergoing radiosurgery, specially in already large tumors.
14
In cystic tumors, rapid clinical worsening is common due to
sudden expansion of cystic elements. Tighter adherences are
found between cystic tumors and surrounding nervous ele-
ments (particularly brainstem and possibly facial nerve) when
compared to solid lesions. Therefore, a wait-and-see policy
is usually not recommended to patients with cystic vestibular
schwannomas. In relation to the surgical technique, careful
sharp dissection to divide the tumor adherences from the ner-
vous tissue must be employed. However, severe complications
may be caused by excessive efforts to dissect the tumor from
brainstem adherences.
4
ARACHNOID CYSTS
Although CPA arachnoid cysts represent a small number of to-
tal arachnoid cysts, the CPA is the second most common loca-
tion for arachnoid cysts to occur, secondary only to the sylvian
fissure. These congenital lesions are usually found in children
who are either asymptomatic or present with subtle signs or
symptoms related to compression of adjacent cerebral and neu-
rovascular structures.
34
Arachnoid cysts are smoothly marginated, presenting CSF-
like signal intensity in all MRI imaging sequences and do not
enhance after contrast administration (Fig. 4). Arachnoid cysts
may be much similar to epidermoid cysts in their radiological
features, especially in the CPA.
10
It is essential, therefore, to di-
fferentiate the two lesions because they may warrant different
therapeutic interventions. Both lesions are characteristically
well-demarcated and have a homogeneous low-density, simi-
lar to cerebrospinal fluid on CT scan, presenting no contrast
enhancement. On MRI, both epidermoids and arachnoid cysts
appear hypointense on T1-weighted images and hyperintense
on T2-weighted images. On FLAIR, however, an arachnoid
cyst tends to follow the cerebrospinal fluid intensity, whereas
an epidermoid tumor becomes strongly hyperintense. Howe-
ver, a few times, an epidermoid may appear as a low-intensity
lesion on FLAIR. This dilemma is solved with the use of echo
planar diffusion scanning, in which an epidermoid cyst remains
bright, while arachnoid cyst not.
12
Reviso
J Bras Neurocirurg 22 (3): 66-71, 2011
Mattei TA, Goulart CR, Lima JS, Ramina R - Differential Diagnosis and Surgical Management of Cerebellopontine Angle Cystic Lesions
69
Figure 4. MRI sequences demonstrating a large (5,5 x 4,5 x 4,0) cystic CPA le-
sion without extension in the internal acoustic canal. The lesion does not present
contrast-enhancement nor displaces the VII/VIII nerves, a common finding of ara-
chnoid cysts.
Not all arachnoid cysts require surgical intervention.
29
Patients
with asymptomatic cysts should be followed clinically and
radiologically with sequential MRI. Indications for operative
management include lesions that demonstrate growth, neural
compression, hydrocephalus or refractory symptoms that may
be related to cysts in this location, such as auditory loss or ce-
rebellar signs.
2
The definitive treatment for arachnoid cysts still remains cra-
niotomy and microsurgical resection or fenestration of the cyst
walls, usually through a retrosigmoid suboccipital approach.
28
More recently, some authors have endoscopic cisternostomy
through a single key-hole, as a minimally invasive approach.
21
An alternative would be the insertion of a cyst-peritoneal
shunt, but the high incidence of shunt malfunction demanding
a second shunt review operation and the relatively good results
using the marsupialization, make it second-line modality of
treatment for arachnoid cysts, especially in the CPA.
21
CYSTIC MENINGIOMAS
Meningiomas are the second most common tumors of the CPA
after vestibular schwannomas, comprising 6 to 15% of cases
of CPA lesions. However, cystic meningiomas in the CPA are
much rarer. These tumors usually appear oval or hemispheric,
with broad dural-based attachments to the tentorium or petrous
bone dura. Commonly there is a solid component, which de-
monstrates marked contrast- enhancement.
12
Usually no ex-
tension into the internal auditory canal is noted.
15
The surgical
resection of such tumors is in general easier when compared
to vestibular schwannomas (unless there is a presence of hard
component) and nerve function preservation rates tends to be
higher.
Meningiomas of the CPA rarely extend into the internal audi-
tory canal (IAC) or arise from its dural lining (approximately
1.7% of all CPA meningiomas and almost all of them non-cys-
tic).
30
The clinical symptoms of intracanalicular meningiomas
are very similar to those of vestibular schwannomas. Most of
the patients reported in the literature, at the time of diagnosis
present with vestibulocochlear nerve disturbances, such as he-
aring loss, tinnitus, disequilibrium and vertigo, or facial nerve
paralysis.
8
These CPA meningiomas involving the IAC require
special surgical management. In most of the patients whose
tumor arises from the dura within the IAC, facial and cochlear
nerve preservation is much more difficult to be achieved, be-
cause of the infiltrative behavior of such lesions.
16
RARE LESIONS
Neurocysticercosis
Although the brain parenchyma is regarded as the most usual
site of involvement of neurocysticercosis, certain reports claim
that subarachnoid space is main location for such lesions. If
the larvae lodge in the meningeal layers, the infestation may
involve the subarachnoid space.
5
Such subarachnoid cysts may
become multi-loculated, resembling a cluster of grapes. This
is usually referred as the racemose form of neurocysticerco-
sis. Within the subarachnoid space, the CPA and suprasellar
cisterns are the most common locations.
38
On MRI, these le-
sions show the same signal intensity as the CSF on all pulse
sequences, with no post-contrast enhancement.
The diffuse infestation observed in some racemose forms can
sometimes be difficult to be distinguished from the surroun-
ding CSF space. The clue to the presence of such lesions is the
focal widening of the CSF space or secondary inflammatory
response in the adjacent parenchyma. Infestation of the suba-
rachnoid space may also result in communicating hydrocepha-
lus due to chronic meningitis. Additionally MRI may show
enhancement of the subarachnoid cisterns due to inflammatory
response.
Reviso
J Bras Neurocirurg 22 (3): 66-71, 2011
Mattei TA, Goulart CR, Lima JS, Ramina R - Differential Diagnosis and Surgical Management of Cerebellopontine Angle Cystic Lesions
70
It is important to identify cysticercotic cysts and to differentiate
them from other tumoral types of CPA cystic lesion
35
, because
the best therapeutic option for most of the patients still remains
the pharmacological treatment against the larvae. In most of
the cases, especially in subarachnoid infestation, supplemen-
tary steroids are recommended to avoid an abrupt immune
response. In selected cases, if there is evidence of CSF flow
obstruction, surgical removal of the cyst may be indicated.
Neuroenteric Cysts
Neurenteric or enterogenous cysts are lesions lined with mu-
cin-secreting and/or ciliated, cuboidal or columnar epithelium,
resembling that found in the respiratory and intestinal tract.
They result from the inappropriate partitioning of the embryo-
nic notochordal plate and presumptive endoderm during the
third week of human development. These lesion have been
described with several different terms, including endodermal,
foregut, epithelial, bronchogenic, and respiratory cysts.
7
Most
commonly, they are encountered as an intradural extramedulla-
ry cyst, especially in the lower cervical and upper thoracic re-
gions and are usually associated with dysraphism.
Neurenteric cysts arising intracranially are rare and to date only
53 cases have been described in the literature, 92% of which
were located in the posterior fossa, most of them as solitary
lesions. These cysts tend to present a slight male predominance
(60% of the cases) as well as a wide range of age of presenta-
tion - from birth to 77 years (mean 34 years).
3
Clinical symp-
toms are usually non-specific and result from inflammatory
response or local mass effect. The most frequent symptoms are
headache and gait disturbances. Our literature search yielded
only 15 cases of neurenteric cysts located in the CPA.
1
Similar
to other lesions at this location, the reported neurenteric cysts
may also present clinically involving cranial nerve deficits.
Surgical resection is the most indicated therapy for most of
the lesions. Intra-operatively these tumors are usually found to
have a dark-red appearance, containing muddy gelatinous fluid
in its multi-cystic compartments. The surrounding dura may be
thick and yellowish because of reactive hypervascularization.
19
Although very rare in this location, this benign developmen-
tal lesion should also be considered as a potential differential
diagnosis for patients presenting with cystic lesions in the CPA.
Other lesions
There have been several isolated case reports of other cystic
lesions in the CPA, such as: cavernous malformation
37,39
, Ec-
cordosis physaliphora lesion
41
(an uncommon benign lesion
originating from embryonic notochordal remnants), as well
as other rare malignant tumors - such as anaplastic ganglio-
glioma
22
, primary epidermoid carcinoma
13
, endolymphatic sac
tumor
27
, primary atypical teratoid/rhabdoid tumor
42
. The cystic
appearance of the malignant lesions is thought to be origina-
ted from intra-tumoral necrosis leading to cystic degeneration.
For most of them, surgical treatment is still the first option of
treatment, having the advantage of also providing histological
sample for analysis.
CONCLUSIONS
Although cystic schwannomas are still the most common cys-
tic lesions of the CPA, a careful preoperative analysis is recom-
mended, when evaluating a cystic lesion in the CPA. The wide
range of possible differential diagnosis includes: epidermoid
cyst, arachnoid cyst, cystic meningioma as well as other rare
entities such as neurocysticercosis, neurenteric cysts, and vas-
cular and malignant cystic tumors.
Surgical management is the mainstay treatment for the majori-
ty of such lesions, with the theoretical advantage of providing
histological sample for confirmation of suspected diagnosis.
As we have previously discussed elsewhere, although the clas-
sic retrosigmoid route remains the standard surgical approach
to CPA lesions, the surgical technique should be tailored to
each specific case according to particularities of patients ana-
tomy as well as lesion appearance and nature.
23
REFERENCES
1. Akaishi K, Hongo K, Ito M, Tanaka Y, Tada T, Kobayashi S.
Endodermal cyst in the cerebellopontine angle with immuno-
histochemical reactivity for CA19-9. Clin Neuropathol 2000;
19(6):296-9.
2. Becker T, Wagner M, Hofmann E, Warmuth-Metz M, Nadjmi
M. Do arachnoid cysts grow? A retrospective volumetric study.
Neuroradiology 1991; 33(4):341-5.
3. Bejjani GK, Wright DC, Schessel D, Sekhar LN. Endodermal
cysts of the posterior fossa: report of three cases and review of
literature. J Neurosurg 1998; 89(2):326-35.
4. Benech F, Perez R, Fontanella MM, Morra B, Albera R, Ducati
A. Cystic versus solid vestibular schwannomas: a series of 80
grade III-IV patients. Neurosurg Rev. 2005; 28(3):209-13.
5. Celis MA, Mourier KL, Polivka M, Boissonnet H, Kato T, Lot
G, George B, et al. Cisternal cysticercosis of the cerebellopon-
tine angle. Neurochirurgie 1992; 38(2):108-12.
6. Charabi S, Tos M, Brgesen SE, Thomsen J. Cystic acoustic
neuromas. Results of translabyrinthine surgery. Arch Otolaryn-
gol Head Neck Surg. 1994; 120(12):1333-8.
7. Chaynes P, Bousquet P, Sol JC, Delisle MB, Richaud J, Lagarri-
gue J. Recurrent intracranial neuroenteric cysts. Acta Neurochir
(Wien) 1998; 140(9):905-11.
8. Dazert S, Aletsee C, Brors D, Mlynski R, Sudhoff H, Hildmann
H, et al. Rare tumors of the internal auditory canal. Eur Arch
Otorhinolaryngol 2005; 262(7):550-4.
9. Dechambre S, Duprez T, Lecouvet F, Raftopoulos C, Gosnard
G. Diffusion-weighted MRI postoperative assessment of an epi-
dermoid tumour in the cerebellopontine angle. Neuroradiology
1999; 41(11):829-31.
10. Dutt SN, Mirza S, Chavda SV, Irving RM. Radiologic differen-
tiation of intracranial epidermoids from arachnoid cysts. Otol
Neurotol 2002; 23(1):84-92.
Reviso
J Bras Neurocirurg 22 (3): 66-71, 2011
Mattei TA, Goulart CR, Lima JS, Ramina R - Differential Diagnosis and Surgical Management of Cerebellopontine Angle Cystic Lesions
71
11. Gao PY, Osborn AG, Smirniotopoulos JG, Harris CP. Radiolog-
ic-pathologic correlation. Epidermoid tumor of the cerebello-
pontine angle. AJNR Am J Neuroradiol 1992; 13(3):863-72.
12. Hakyemez B, Yildiz H, Ergin N, Uysal S, Parlak M. Flair and
diffusion weighted MR imaging in differentiating epidermoid
cysts from arachnoid cysts. Tani Girisim Radyol 2003; 9(4):418-
26.
13. Ishikawa S, Yamazaki M, Nakamura A, Hanyu N. An autopsy
case of primary cerebellar-pontine angle epidermoid carcinoma.
Rinsho Shinkeigaku 2000; 40(3):243-8.
14. Iwai Y, Yamanaka K, Yamagata K, Yasui T. Surgery after radio-
surgery for acoustic neuromas: surgical strategy and histological
findings. Neurosurgery 2007; 60(2 Suppl 1):ONS75-82; discus-
sion ONS82.
15. Jallo GI, Woo HH, Meshki C, Epstein FJ, Wisoff JH. Arachnoid
cysts of the cerebellopontine angle: diagnosis and surgery. Neu-
rosurgery 1997; 40(1):31-7; discussion 37-8.
16. Jeng CM, Huang JS, Lee WY, Wang YC, Kung CH, Lau MK.
Magnetic resonance imaging of acoustic schwannomas. J For-
mos Med Assoc 1995; 94(8):487-93.
17. Kameyama S, Tanaka R, Kawaguchi T, Fukuda M, Oyanagi K.
Cystic acoustic neurinomas: studies of 14 cases. Acta Neurochir
(Wien) 1996; 138(6):695-9.
18. Kawamura Y, Sze G. Totally cystic schwannoma of tenth cranial
nerve mimicking an epidermoid. AJNR Am J Neuroradiol 1992;
13(5):1333-4.
19. Kumar R, Nayak SR. Unusual neuroenteric cysts: diagnosis and
management. Pediatr Neurosurg 2002; 37(6):321-30.
20. Kwon Y, Khang SK, Kim CJ, Lee DJ, Lee JK, Kwun BD. Ra-
diologic and hispopathologic changes after gamma knife radio-
surgery for acoustic schwannoma. Stereotact Funct Neurosurg
1999; 72 Suppl 1:2-10.
21. Marin-Sanabria EA, Yamamoto H, Nagashima T, Kohmura E.
Evaluation of the management of arachnoid cyst of the posterior
fossa in pediatric population: experience over 27 years. Childs
Nerv Syst. 2007; 23(5): 535-42.
22. Matsuzaki K, Uno M, Kageji T, Hirose T, Nagahiro S. Anaplas-
tic ganglioglioma of the cerebellopontine angle. Case report.
Neurol Med Chir (Tokyo) 2005; 45(11):591-5.
23. Mattei TA, Ramina R. Critical remarks on the proposed extend-
ed retrosigmoid approach. Neurosurg Rev. 2011; 34(4):527-30.
24. Miyagi A, Maeda K, Sugawara T. Large cystic neurinoma: a
case report. No Shinkei Geka 1997; 25(7):647-54.
25. Nakamura M, Roser F, Mirzai S, Matthies C, Vorkapic P, Samii
M. Meningiomas of the internal auditory canal. Neurosurgery
2004; 55(1):119-27; discussion 127-8.
26. Ochi M, Hayashi K, Hayashi T, Morikawa M, Ogino A, Hash-
mi R, et al. Unusual CT and MR appearance of an epidermoid
tumor of the cerebellopontine angle. AJNR Am J Neuroradiol
1998; 19(6):1113-5.
27. Ouallet JC, Marsot-Dupuch K, Van Effenterre R, Kujas M, Tu-
biana JM. Papillary adenoma of endolymphatic sac origin: a
temporal bone tumor in von Hippel-Lindau disease. Case report.
J Neurosurg 1997; 87(3):445-9.
28. Pradilla G, Jallo G.. Arachnoid cysts: case series and review of
the literature. Neurosurg Focus 2007; 22(2):E7.
29. Punzo A, Conforti R, Martiniello D, Scuotto A, Bernini FP, Ci-
offi FA. Surgical indications for intracranial arachnoid cysts.
Neurochirurgia (Stuttg) 1992; 35(2):35-42.
30. Roser F, Nakamura M, Dormiani M, Matthies C, Vorkapic P,
Samii M. Meningiomas of the cerebellopontine angle with
extension into the internal auditory canal. J Neurosurg 2005;
102(1):17-23.
31. Safavi-Abbasi S, Di Rocco F, Bambakidis N, Talley MC, Ghar-
abaghi A, Luedemann W, et al. Has management of epidermoid
tumors of the cerebellopontine angle improved? A surgical syn-
opsis of the past and present. Skull Base 2008; 18(2):85-98.
32. Sarrazin J, Hlie O, Cordoliani Y. Cerebellopontine angle tu-
mors in adults. J Radiol. 2000; 81(6 Suppl):675-90.
33. Savader SJ, Murtagh FR, Savader BL, Martinez CR. Magnetic
resonance imaging of the intracranial epidermoid tumors. Clin
Radiol 1989; 40(3):282-5.
34. Shenouda EF, Moss TH, Coakham HB. Cryptic cerebellopon-
tine angle neuroglial cyst presenting with hemifacial spasm.
Acta Neurochir (Wien) 2005; 147(7):787-9; discussion 789.
35. Singh S GS, Bannur U, Chacko G, Korah IP, Rajshekhar V. Cys-
ticercosis of the cerebellopontine angle cistern mimicking epi-
dermoid inclusion cyst. Acta Neurol Scand 1999; 99(4):260-3.
36. Steffey DJ, De Filipp GJ, Spera T, Gabrielsen TO. MR imaging
of primary epidermoid tumors. J Comput Assist Tomogr. 1988;
12(3):438-40.
37. Stevenson CB, Johnson MD, Thompson RC. Cystic cavernous
malformation of the cerebellopontine angle. Case illustration. J
Neurosurg. 2005; 103(5):931.
38. Takayanagui OM, Odashima NS. Clinical aspects of neurocysti-
cercosis. Parasitol. Int 2006; 55(suppl):111-115.
39. Vajramani GV, Devi BI, Hegde T, Srikanth SG, Shankar SK.
Cystic cavernous malformation of the cerebellopontine angle.
Clin Neurol Neurosurg. 1998; 100(2):133-7.
40. Vinchon M, Pertuzon B, Lejeune JP, Assaker R, Pruvo JP, Chris-
tiaens JL. Intradural epidermoid cysts of the cerebellopontine
angle: diagnosis and surgery. Neurosurgery 1995; 36(1):52-6;
discussion 56-7.
41. Watanabe A, Yanagita M, Ishii R, Shirabe T. Magnetic reso-
nance imaging of ecchordosis physaliphora--case report. Neurol
Med Chir (Tokyo) 1994; 34(7):448-50.
42. Weyers SP, Khademian ZP, Biegel JA, Chuang SH, Korones DN,
Zimmerman RA. Primary intracranial atypical teratoid/rhabdoid
tumors of infancy and childhood: MRI features and patient out-
comes. AJNR Am J Neuroradiol 2006; 27(5):962-71.
CORRESPONDING AUTHOR
Tobias Alecio Mattei, M.D 828
Northeast Glen Oak Ave ap. 304
ZIP 61603-3285Peoria/IL
e-mail: tobias.a.mattei@osfhealthcare.org
Você também pode gostar
- Artigo MaláriaDocumento12 páginasArtigo MaláriaOctávio Augusto Cruz BritoAinda não há avaliações
- Causas de Distensão Na Panturrilha e Opções de TRDocumento1 páginaCausas de Distensão Na Panturrilha e Opções de TRPedro RochaAinda não há avaliações
- Tipagem SanguineaDocumento5 páginasTipagem SanguineaGelma RochaAinda não há avaliações
- Estudo Dirigido de ImunologiaDocumento6 páginasEstudo Dirigido de ImunologiaMárcio JorqueraAinda não há avaliações
- Condições Infecciosas Mais Prevalentes em Ginecologia em Nível Ambulatoria - 14 - 09 - OsvaniDocumento21 páginasCondições Infecciosas Mais Prevalentes em Ginecologia em Nível Ambulatoria - 14 - 09 - OsvaniClaudia FreireAinda não há avaliações
- Bronquiolite Diretrizes para o Diagnóstico, Tratamento e PrevençãoDocumento10 páginasBronquiolite Diretrizes para o Diagnóstico, Tratamento e PrevençãoVitor CathcartAinda não há avaliações
- Ca de EndométrioDocumento44 páginasCa de EndométrioDiêgo ArgôloAinda não há avaliações
- Prevenir e Tratar As Alergias ExcertoDocumento8 páginasPrevenir e Tratar As Alergias ExcertoMarco CruzAinda não há avaliações
- Questionário Minerais 10-05-21Documento3 páginasQuestionário Minerais 10-05-21EstudosAinda não há avaliações
- ASMA Clinica MedicaDocumento50 páginasASMA Clinica MedicaAline MostaroAinda não há avaliações
- Plano de Aula CancerDocumento2 páginasPlano de Aula CancerAnna RemorAinda não há avaliações
- Insuficiência CardíacaDocumento28 páginasInsuficiência CardíacaGeovanni MoraisAinda não há avaliações
- Controle de Infeccao Parte IDocumento95 páginasControle de Infeccao Parte INatalia VanessaAinda não há avaliações
- Acupuntura No Tratamento Da Hernia UmbilicalDocumento30 páginasAcupuntura No Tratamento Da Hernia UmbilicalNarya OlórinAinda não há avaliações
- Relatorio Cadeira de RodasDocumento1 páginaRelatorio Cadeira de Rodasveniciosantos.ce100% (1)
- Exercicio GasometriaDocumento3 páginasExercicio GasometriaItana NogueiraAinda não há avaliações
- Síndrome Coronariana Aguda e Infarto Agudo Do Miocárdio - Morfo1m1Documento22 páginasSíndrome Coronariana Aguda e Infarto Agudo Do Miocárdio - Morfo1m1elisaAinda não há avaliações
- DengueDocumento4 páginasDengueS2S212340% (1)
- 3-Microbiologia Vírus e BactériasDocumento52 páginas3-Microbiologia Vírus e BactériasDenivaldo Silva FerreiraAinda não há avaliações
- Plano de Estudo Marica RJDocumento15 páginasPlano de Estudo Marica RJdanielgomesalvesdacruz0% (1)
- Bovino de LeiteDocumento12 páginasBovino de LeiteRaul JuniorAinda não há avaliações
- Angina Estável (Mapa Mental)Documento1 páginaAngina Estável (Mapa Mental)Elcio Fernando MachowskiAinda não há avaliações
- Interpretação Da Gasometria ArterialDocumento2 páginasInterpretação Da Gasometria ArterialMariana Magnoni PeriardAinda não há avaliações
- AmoxilinaDocumento2 páginasAmoxilinaSABRINA SENAAinda não há avaliações
- Licenças de Produtos No Brasil 05-2013Documento196 páginasLicenças de Produtos No Brasil 05-2013Paulo AndreoliAinda não há avaliações
- Depressão SazonalDocumento3 páginasDepressão SazonalGê PinkerAinda não há avaliações
- AsdDocumento496 páginasAsdGiovanniCisottoAinda não há avaliações
- TAMOXIFENODocumento3 páginasTAMOXIFENOGuilherme GurgelAinda não há avaliações
- 1 - Desafio Atencao Pediatrica PDFDocumento13 páginas1 - Desafio Atencao Pediatrica PDFEliane SenaAinda não há avaliações
- Fmurologiabelemafv 01Documento12 páginasFmurologiabelemafv 01Jose Morato E FlavianeAinda não há avaliações