Escolar Documentos
Profissional Documentos
Cultura Documentos
Gradiente SP2
Enviado por
JoséTítulo original
Direitos autorais
Formatos disponíveis
Compartilhar este documento
Compartilhar ou incorporar documento
Você considera este documento útil?
Este conteúdo é inapropriado?
Denunciar este documentoDireitos autorais:
Formatos disponíveis
Gradiente SP2
Enviado por
JoséDireitos autorais:
Formatos disponíveis
Rev Bras Anestesiol ARTIGO CIENTÍFICO
2001; 51: 4: 305 - 310 SCIENTIFIC ARTICLE
Gradiente SpO2 - SaO2 Durante Ventilação Mecânica em
Anestesia e Terapia Intensiva *
SpO2 - SaO2 Gap During Mechanical Ventilation in
Anesthesia and Intensive Care
Pablo Escovedo Helayel 1, Getúlio R. de Oliveira Filho, TSA 2, Lúcia Marcon 3, Flávio Hülse Pederneiras 4,
Marcos Antônio Nicolodi, TSA 5, Sérgio Galluf Pederneiras, TSA 6
RESUMO pares analisados, somente valores acima de 99% excluíram
Helayel PE, Oliveira Filho GR, Marcon L, Pederneiras FH, Nico- pacientes com SaO2 menor que 90%.
lodi MA, Pederneiras SG - Gradiente SpO2 - SaO2 Durante Ven- UNIT ERMOS: MONITORIZAÇÃO: oximetria de pulso;
tilação Mecânica em Anestesia e Terapia Intensiva VENTILAÇÃO: ventilação mecânica
Justificativas e Objetivos - A saturação periférica da SUMMARY
oxihemoglobina (SpO2) é freqüentemente utilizada para guiar Helayel PE, Oliveira Filho GR, Marcon L, Pederneiras FH, Nico-
alterações do regime ventilatório. Valores de SpO2 iguais ou lodi MA, Pederneiras SG - SpO2 - SaO2 Gap During Mechanical
superiores a 96% são necessários para garantir saturação ar-
Ventilation in Anesthesia and Intensive Care
terial da oxihemoglobina (SaO 2 ) superiores a 90%, em
pacientes de terapia intensiva. Este estudo teve por objetivo
determinar concordância entre valores de SpO2 e SaO2 e Background and Objectives - Peripheral oxy-hemoglobin sat-
delimitar a menor SpO2 associada a valores de SaO2 iguais ou uration (SpO2) is commonly used to guide ventilator settings.
superiores a 90%. SpO2 values equal to, or higher than 96% are necessary to as-
Método - Foram incluídos prospectivamente 120 pacientes sure arterial oxy-hemoglobin saturation (SaO2) higher than
adultos, de ambos os sexos, submetidos à anestesia geral com 90% in intensive care patients. This study aimed to determine
ventilação mecânica ou em tratamento intensivo. Amostras de SpO2 - SaO2 gap and to establish the lowest SpO 2 associated to
sangue arterial foram coletadas por punção arterial ou por SaO2 values equal to, or higher than 90%.
aspiração de linha arterial, utilizando técnica anaeróbia, em se- Methods - Participated in this prospective study 120 adult pa-
ringas heparinizadas. As amostras foram analisadas tients of both genders submitted to general anesthesia and me-
imediatamente após a coleta. A SpO2 foi medida por oxímetro chanical ventilation or under intensive care. Arterial blood
de pulso durante a coleta, no indicador da mão contra-lateral, samples were obtained by arterial puncture or central line aspi-
utilizando a onda dicrótica de pulso arterial como parâmetro de ration using the anaerobic technique and heparin-containing
adequação. syringes. Samples were analyzed immediately after collection.
Resultados - Foram analisadas 228 amostras. A diferença en- SpO2 was measured during collection with the pulse oximeter
tre os valores de SpO2 e SaO2 variou entre -7,10% e 15,20%, placed on the opposite second finger and using arterial pulse
sendo a diferença média igual a -0,20% ± 2,02%. SpO2-SaO2 dichroic wave as the adequacy parameter.
maiores que 4,04% (dois desvios padrão da diferença) Results - Two hundred and twenty-eight samples were ana-
ocorreram em 4,72% das amostras. A determinação gráfica da lyzed. The difference between SpO2 and SaO2 ranged between
SpO2, mínima para garantir a SaO2 acima de 90%, mostrou que -7.10% and 15.2%, being -0.20% ± 2.02% the mean difference
somente valores de SpO2 iguais ou superiores a 99% não se (bias). SpO2-SaO2 higher than 4.04% (two standard deviations
associaram à ocorrência de nenhum valor de SaO2 inferior a of the difference) was observed in 4.72% of samples. Graphical
90%. analysis of the lowest SpO2 to assure an SaO2 higher than 90%
Conclusões - Embora a diferença entre os valores de SpO2 e has shown that only SpO2 values equal to, or higher than 99%
SaO2 tenham se localizado entre mais e menos 5% em 97% dos were not associated to SaO2 values below 90%.
Conclusions - Although SpO2-SaO2 gap remaining between
plus or minus 5% for 97% of the samples, only SpO 2 values
higher than 99% excluded patients with SaO2 values below
* Recebido do (Received from) Hospital Governador Celso Ramos - 90%.
CET/SBA Integrado de Anestesiologia da SES-SC, Florianópolis, SC
KEY WORDS - MONITORING: pulse oximetry; VENTILATION:
1. ME2 do CET/SBA da SES-SC mechanical ventilation
2. Responsável pelo CET/SBA da SES-SC
3. Enfermeira da Unidade de Tratamento Intensivo
4. ME1 do CET/SBA da SES-SC INTRODUÇÃO
5. Anestesiologista do Hospital Governador Celso Ramos
6. Co-Responsável do CET/SBA da SES-SC
saturação periférica da oxihemoglobina é uma estimati-
Apresentado (Submitted) em 01 de dezembro de 2000
Aceito (Accepted) para publicação em 09 de janeiro de 2001
A va de sua saturação no sangue arterial amplamente uti-
lizada na monitorização de pacientes durante anestesia e
Correspondência para (Mail to): em terapia intensiva. Durante ventilação mecânica, a SpO 2
Dr. Getúlio Rodrigues. de Oliveira Filho tem sido utilizada para determinar a adequação de mudan-
Rua José Cândido Silva 179/402
88075-250 - Florianópolis, SC
ças feitas no regime ventilatório, como alterações da fração
E-mail: grof@th.com.br inspirada de oxigênio, valores de pressão positiva tele-expi-
ratória e desmame. Os valores de SpO 2 tradicionalmente
Ó Sociedade Brasileira de Anestesiologia, 2001
Revista Brasileira de Anestesiologia 305
Vol. 51, Nº 4, Julho - Agosto, 2001
HELAYEL, OLIVEIRA FILHO, MARCON E COLS
associados com SaO 2 acima de 90%, ou seja, normoxemia, Tabela I - Dados Demográficos
variam entre 92 e 94% 1 . Entretanto, recentemente, a au- Idade (anos) * 52,94 ± 16,56
sência de hipoxemia só foi verificada quando os valores da Sexo #
SpO 2 foram iguais ou maiores que 96% 2 . Estes achados
Masculino 66
possuem implicações clínicas óbvias.
Este estudo teve como objetivos estudar os limites de con- Feminino 54
cordância entre os valores de SpO 2 e SaO 2 em pacientes Peso (kg) * 71,60 ± 15,97
anestesiados e criticamente enfermos durante ventilação Altura (m) * 1,65 ± 0,09
mecânica e estabelecer os valores mínimos de SpO2 associa-
* Valores expressos pela Média ± DP
dos a saturações arteriais da oxihemoglobina superiores a # Número de casos
90%.
Tabela II - Comparação entre os Valores de SaO 2 e SpO 2
Mediana [quartil inf.; superior]
MÉTODO Parâmetro (Mínimo - Máximo)
SaO2 99,8 [98,5; 100] *
Com a aprovação da Comissão de Ética Médica do Hospital 83 - 100
Governador Celso Ramos, foram incluídos prospectivamen- SpO2 99 [98;100]
te 120 pacientes adultos, de ambos os sexos, submetidos à 84 - 100
ventilação mecânica durante anestesia geral ou terapia in- * p < 0,05 comparado à SpO2
tensiva, com fração inspirada de oxigênio entre 40% e 100%,
independentemente dos demais parâmetros de ventilação
utilizados ou do estado hemodinâmico. Foram excluídos os 18,18
pacientes em circulação extracorpórea, os ictéricos, os que 16,16
14,14
tinham esmalte nas unhas e os anêmicos (hemoglobina me- 12,12
SpO 2 - SaO 2
10,10
nor que 9 g.ml-1 ). Também não foram incluídos pacientes cu- 8,08
6,06
jas gasometrias apresentaram SaO 2 igual ou menor que 4,04
2,02
75%, por possibilidade de contaminação venosa da amostra 0
-2,02
durante a punção arterial. Amostras de sangue arterial foram -4,04
-6,06
coletadas por punção da artéria radial ou por aspiração de li- -8,08
-10,10
nha arterial, utilizando técnica anaeróbia, em seringas hepa- 86 88 90 92 94 96 98 100 102
rinizadas. As amostras foram analisadas imediatamente Média
após a coleta. Durante a coleta, foram anotados os valores
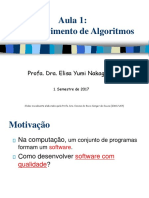
de SpO 2 , a partir de oxímetro de pulso com sensores reutili- Figura 1 - Diagrama do Bland-Altman para a SpO2 - SaO 2
záveis digitais, utilizando a onda dicrótica de pulso arterial
como parâmetro de adequação da medida.
Os valores de SpO2 e de SaO 2 foram comparados pelo teste
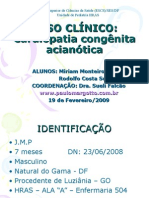
U de Mann-Whitney e sua concordância foi avaliada pelo mé- A determinação gráfica da SpO 2 mínima para garantir a SaO 2
todo de Bland-Altman. Para determinar o menor valor de acima de 90% mostrou que somente valores de SpO 2 iguais
SpO 2 associado com SaO 2 igual ou superior a 90%, foi utiliza- ou superiores a 99% não se associaram à ocorrência de ne-
do um gráfico SaO 2 , SpO 2 no qual foram desenhadas duas li- nhum valor de SaO 2 inferior a 90% (Figura 2).
nhas. A primeira linha, vertical, definiu o limite de SaO 2 em
90% e a segunda, horizontal, cruzou o eixo das ordenadas no
valor de SpO 2 acima do qual não foram observados valores
de SaO 2 menor que de 90%. 100
99
98
97
96
95
RESULTADOS
SpO 2
94
93
92
91
Foram analisadas 228 amostras de 120 pacientes cujos 90
89
dados demográficos estão representados na tabela I. Os 88
87
valores de SpO 2 diferiram significativamente dos da SaO 2 86
85
(Tabela II). A diferença entre os valores de SpO 2 e SaO 2 va- 84
82 84 86 88 90 92 94 96 98 100 102
riou entre -7.10% e 15,20%, sendo a diferença média igual
SaO 2
a - 0,20%, com desvio padrão igual a 2,02%. O gradiente
SpO 2 - SaO 2 localizou-se entre menos e mais 4,04% (dois
desvios padrão da diferença média) em 95,28% das amos- Figura 2 - Determinação Gráfica do Valor Mínimo da SpO2 para Evi-
tras (Figura 1). tar SaO2 menor que 90%
306 Revista Brasileira de Anestesiologia
Vol. 51, Nº 4, Julho - Agosto, 2001
SPO2 - SAO2 GAP DURING MECHANICAL VENTILATION IN ANESTHESIA AND INTENSIVE CARE
DISCUSSÃO Fatores demográficos, como idade, sexo ou raça não influen-
ciam a relação entre a SpO2 e SaO2 13. Em negros, SpO2 abai-
O diagnóstico clínico de hipoxemia é dado pela presença de xo de 95% reflete SaO2 menor que 90%, enquanto, em bran-
cianose. Entretanto, esta somente ocorre quando a SaO 2 é cos, o valor correspondente da SpO2 é 92% 6.
menor que 75% e depende da concentração de hemoglobina Os valores normais do gradiente SpO2 - SaO 2 variam entre
reduzida, que deve ser superior a 5 g.dl-1 . Assim, sua ausên- menos e mais 3 a 5% 6 .
cia não elimina a possibilidade de hipoxemia 1 . A saturação Em anestesia e, especialmente em terapia intensiva, a SpO 2
periférica da oxihemoglobina correlaciona-se fortemente é utilizada para indicar alterações do regime ventilatório.
com a saturação arterial da oxihemoglobina e, por esta razão Assumindo valores normais do gradiente SpO 2 - SaO 2 , utili-
é utilizada rotineiramente na monitorização peri-operatória e zam-se limites inferiores de SpO 2 entre 92 e 94% para evitar
na terapia intensiva, permitindo o diagnóstico precoce de hi- SaO 2 inferior a 90%, que corresponde à hipoxemia leve 3-6 .
poxemia 3,5 . Entretanto, em pacientes criticamente enfermos, sob venti-
Os oxímetros de pulso aferem a diferença na absorção de lação mecânica, o limite inferior da SpO 2 deveria ser de 96%,
dois comprimentos de onda luminosa durante sua passagem para evitar hipoxemia durante alterações do regime ventila-
através de tecidos perfundidos, analisando a faixa de absor- tório 2 .
bância dos componentes contínuo e pulsátil do fluxo sangüí- Neste estudo, 95,28% dos pacientes apresentaram valores
neo tecidual. As taxas de absorbância são relacionadas com do gradiente SpO 2 - SaO 2 , dentro de dos limites de discor-
medidas diretas de SaO 2 obtidas em voluntários sadios por dância, isto é, dois desvios padrão acima e abaixo da diferen-
co-oximetria, resultando em um algoritmo de calibração, que ça média mas 4,72% apresentaram valores excessivamente
é armazenado no microprocessador digital do oxímetro de altos. Nestes, caso a SpO 2 mínima aceitável para afastar hi-
pulso. Assim, é gerada uma estimativa da SaO 2 6 . poxemia durante ajuste do regime ventilatório fosse estipu-
Asaturação de oxigênio da oxihemoglobina no sangue arteri- lada entre 92 e 94%, teriam resultado valores de SaO 2 muito
al pode ser classificada em fracional e funcional. A primeira é abaixo de 90% e os pacientes estariam hipoxêmicos após a
medida espectrofotometricamente pela co-oximetria, sendo intervenção.
calculada pela relação [HbO 2 /(HbO 2 + Hb reduzida + mete- Conclui-se que, embora a SpO 2 estime a SaO 2 com pequena
moglobina + carboxi-hemoglobina) x 100]. A saturação de discordância na grande maioria dos pacientes, somente va-
oxigênio funcional da oxihemoglobina é estimada pela oxi- lores iguais ou maiores que 99% afastam a possibilidade de
metria de pulso e é calculada pela razão [HbO 2 /(HbO 2 + Hb SaO 2 abaixo de 90% em pacientes cirúrgicos ou gravemente
reduzida) x 100] 7 . Desta maneira, a oximetria de pulso não enfermos. Recomenda-se que alterações do regime ventila-
diferencia a hemoglobina reduzida das demais formas de he- tório sejam feitas somente após confirmação gasométrica
moglobina, podendo superestimar a SaO2 na presença des- dos valores da PaO 2 e da SaO 2 .
tas 7 .
Artefatos na medida da SpO 2 foram relacionados à diminui-
ção da razão entre a qualidade do sinal e a interferência na
captação. Assim, o uso de vasopressores, a baixa perfusão
tissular e a colocação inadequada do sensor são responsá- SpO2 - SaO2 Gap During Mechanical
veis pela diminuição do sinal, enquanto o movimento e a luz Ventilation in Anesthesia and Intensive
ambiente aumentam a interferência 8 . A diminuição acentua- Care
da da resistência vascular sistêmica pode fazer com que a
SpO 2 subestime a SaO 2 . Em pacientes sépticos, o oxímetro Pablo Escovedo Helayel, M.D., Getúlio R. de Oliveira Filho,
de pulso é sensibilizado pelo fluxo venoso pulsátil, causado M.D., Lúcia Marcon, M.D., Flávio Hülse Pederneiras, M.D.,
pela abertura de fístulas arterio-venosas cutâneas 9 . Embo- Marcos Antônio Nicolodi, M.D., Sérgio Galluf Pederneiras, M.D.
ra a anemia aguda em pacientes não hipoxêmicos não afete
significativamente a precisão da oximetria de pulso 6 , porta- INTRODUCTION
dores de anemia falciforme, em vigência de crise falcêmica,
apresentam valores de SaO 2 superestimado pela SpO 2 , sem Peripheral oxy-hemoglobin saturation is a widely used esti-
entretanto mascarar o diagnóstico de hipoxemia 10,11 . As mate of its saturation in the arterial blood for monitoring pa-
dis-hemoglobinemias podem falsear as medidas da oxime- tients under anesthesia and/or intensive care. During me-
tria de pulso. Destas, a mais comum é a carboxi-hemoglobi- chanical ventilation, SpO 2 has been used to determine the
nemia, associada ao tabagismo crônico e à intoxicação pelo adequacy of changes in ventilator settings, such as oxygen
monóxido de carbono, em que a SaO 2 é superestimada pela inspired fraction, positive tele-expiratory pressure values
SpO 2 7 . Durante metemoglobinemia grave, a SpO 2 man- and weaning. SpO 2 values traditionally associated to SaO2
tém-se constante, em torno de 85%, independentemente do higher than 90%, that is, normoxemia, vary between 92% and
valor da SaO 2 . Metemoglobinemia pode resultar do uso de ni- 94% 1 . Recently, however, the lack of hypoxemia has been
troprussiato de sódio, nitroglicerina, metoclopramida, sul- only observed with SpO 2 values equal to, or higher than 96%.
fas, prilocaína e benzocaína 12 . Such findings have obvious clinical implications.
Revista Brasileira de Anestesiologia 307
Vol. 51, Nº 4, Julho - Agosto, 2001
HELAYEL, OLIVEIRA FILHO, MARCON ET AL
This study aimed to evaluated matching limits between SpO 2 Table II - Comparison between SaO 2 and SpO 2 values
and SaO 2 in anesthetized and critically ill patients during me- Median [lower; upper quartile]
Parameter (Lowest - Highest)
chanical ventilation to establish minimum SpO2 values asso-
ciated to more than 90% arterial oxy-hemoglobin saturation. 99.8 [98.5; 100]*
SaO2
83 - 100
99 [98;100]
METHODS SpO2
84 - 100
After Hospital Governador Celso Ramos Medical Ethics * p < 0.05 as compared to SpO2
Committee approval, participated in this prospective study
120 patients of both genders submitted to mechanical venti-
18.18
lation during general anesthesia or intensive care, with in- 16.16
14.14
spired oxygen fraction between 40% and 100%, regardless of 12.12
SpO 2 - SaO 2
10.10
other ventilation parameters or of hemodynamic status. Pa- 8.08
6.06
tients in cardio-respiratory bypass, icteric, with nail polish or 4.04
anemic (hemoglobin lower than 9 g.ml-1 ) were excluded from 2.02
0
the study. Patients with SaO 2 equal to, or lower than 75% -2.02
-4.04
were also excluded due to the possibility of venous contami- -6.06
-8.08
nation of the sample during arterial puncture. Arterial blood -10.10
samples were collected by radial artery puncture or arterial 86 88 90 92 94 96 98 100 102
Mean
line aspiration using an anaerobic technique and hepa-
rin-containing syringes. Samples were analyzed immedi- Figure 1 - Bland-Altman Diagram for SpO2 - SaO2
ately after collection. During collection, SpO 2 values were ob-
tained with a pulse oximeter with reusable digital sensors, us-
ing the arterial pulse dichroic wave as the adequacy parame-
ter. Lowest SpO 2 to assure an SaO2 higher than 90% has shown
SpO 2 and SaO 2 values were compared by Mann-Whitney U that only SpO 2 values equal to, or higher than 99% were not
test and their matching was evaluated by Bland-Altman test. associated to SaO2 values below 90% (Figure 2).
To determine the lowest SpO 2 value associated to an SaO 2
equal to, or higher than 90% an SaO 2 , SpO 2 chart was used
where two lines were plotted. The vertical line defined SaO 2
limit in 90% and the horizontal line crossed the ordinate axle 100
at an SpO 2 value above which no SaO 2 values below 90% 99
98
97
were observed. 96
95
SpO 2
94
93
92
91
RESULTS 90
89
88
87
Demographics data of 120 patients of whom 228 samples 86
85
were analyzed are shown in table I. SpO2 values were signifi- 84
82 84 86 88 90 92 94 96 98 100 102
cantly different from SaO 2 values (Table II). Differences be-
SaO2
tween SpO2 and SaO 2 varied from -7.10% to 15.20%. Mean
difference was -0.20% with a standard deviation of 2.02%.
SpO 2 - SaO 2 gap remained between plus or minus 4.04% (two Figure 2 - Graphic Representation of Minimum SpO2 Value to Pre-
standard deviations of the difference) in 95.28% of samples vent SaO2 below 90%
(Figure 1).
Table I - Demographics Data
Age (years) * 52.94 ± 16.56
Gender #
DISCUSSION
Masculino 66
Hypoxemia is confirmed by the presence of cyanosis. How-
Feminino 54 ever, it is only seen when SaO2 is lower than 75% and depends
Weight (kg) * 71.60 ± 15.97 on reduced hemoglobin saturation, which must be higher than
Height (m) * 1.65 ± 0.09 5 g.dl-1. So, its absence does not rule out the possibility of
hypoxemia 1 . Peripheral oxy-hemoglobin saturation is
* Values expressed in Mean ± SD
# Number of cases strongly correlated to oxy-hemoglobin arterial saturation and,
308 Revista Brasileira de Anestesiologia
Vol. 51, Nº 4, Julho - Agosto, 2001
SPO2 - SAO2 GAP DURING MECHANICAL VENTILATION IN ANESTHESIA AND INTENSIVE CARE
as such, it is routinely used in perioperative monitoring and in acceptable SpO 2 to rule out hypoxemia during ventilator set-
intensive care units for an early hypoxemia diagnosis 3,5. tings adjustment was established between 92% and 94%,
Pulse oximetry checks the difference in absorption of two SaO 2 values would be well below 90% and patients would be
light wave lengths crossing perfused tissues, by analyzing hypoxemic after the intervention.
the absorbance range of continuous and pulsatile compo- We concluded that, although SpO 2 estimating SaO 2 with a mi-
nents of tissue blood flow. Absorbance rates are related to nor mismatch in most cases, only values equal to, or higher
SaO 2 measurements obtained in healthy volunteers by than 99% rule out the possibility of SaO 2 below 90% in surgi-
co-oximetry, resulting in a calibration algorithm which is cal or critically ill patients. It is recommended that adjust-
stored in the pulse oximeter’s digital microprocessor and ments in ventilator settings should only be done after confir-
generates an SaO 2 estimate 6 . mation of PaO 2 and SaO 2 .
Arterial oxy-hemoglobin oxygen saturation may be classified
as fractional and functional. The first is spectrophotometri-
cally measured by co-oximetry and is calculated by the REFERÊNCIAS - REFERENCES
[HbO 2 /(HbO 2 + reduced Hb + methemoglobin + carboxy-he-
moglobin) x 100] ratio. Functional oxy-hemoglobin oxygen 01. Powell, JF, Menon DK, Jones JG - The effects of hypoxemia and
recommendations for postoperative oxygen therapy. Anaesthe-
saturation is estimated by pulse oximetry and is calculated by
sia, 1996;51:769-772.
the [HbO 2 /(HbO 2 + reduced Hb) x 100] ratio 7 . This way, pulse 02. Seguin P, Le Rouzo A, Tanguy M et al - Evidence for the need of
oximetry does not distinguish reduced hemoglobin from bedside accuracy of pulse oximetry in an intensive care unit. Crit
other forms of hemoglobin and may overestimate SaO 2 7 . Care Med, 2000;28:703-706.
SpO 2 measurements artifacts were related to a decrease in 03. Moller JT, Johannessen NW, Espersen K et al - Randomized
the ratio between signal quality and capturing interference. evaluation of pulse oximetry in 20,802 patients: I. Perioperative
So, the use of vasopressants, the low tissue perfusion and events and postoperative complications. Anesthesiology, 1993;
78:445-453.
the inadequate placement of the sensor are responsible for
04. Jensen L.A, Onyskiw JE, Prasad NG - Meta-analysis of arterial
signal decrease, while movement and room light increase the oxygen saturation monitoring by pulse oximetry in adults. Heart
interference 8 . The marked decrease in systemic vascular re- Lung, 1998;27:387-408.
sistance may lead SpO 2 to underestimate SaO2 . In septic pa- 05. Smith DC - Pulse oximetry in the recovery room. Anaesthesia,
tients, pulse oximeter is sensitized by the pulsatile venous 1989;44:345-348.
flow caused by the opening of skin arterial-venous fistulas 9 . 06. Jubran A - Advances in respiratory monitoring during mechani-
Although acute anemia in non hypoxemic patients does not cal ventilation. Chest, 1999;116:1416-1425.
07. Hampson N - Pulse oximetry in severe carbon monoxide poiso-
significantly affect pulse oximetry precision 6 , sickle cell dis-
ning. Chest, 1998;114:1036-1041.
ease patients during crisis show SaO 2 values underesti-
08. Severinghaus JW, Spellman MJ - Pulse oximeter failure thres-
mated by SpO 2 , however without hiding the diagnosis of holds in hypotension and vasoconstriction. Anesthesiology,
hypoxemia 10,11 . Dyshemoglobulinemias may affect pulse 1990;73:532-537.
oximetry measurements. From those, the most common is 09. Secker C, Spiers P - Accuracy of pulse oximetry in patients with
carboxy-hemoglobulinemia associated to chronic smoking low systemic vascular resistance. Anaesthesia, 1997;52:
and CO 2 poisoning, where SaO 2 is overestimated by SpO 2 . 127-130.
During severe methemoglobinemia, SpO 2 is constant around 10. Kress JP, Pohlman AS, Hall JB - Determination of hemoglobin
saturation in patients with acute sickle chest syndrome: a com-
85%, regardless of SaO 2 . Methemoglobulinemia may result
parison of arterial blood gases and pulse oximetry. Chest,
from the use of sodium nitroprusside, nitroglycerin, 1999;115:1316-1320.
metoclopramide, sulfas, prilocaine and benzocaine 12 . 11. Ortiz FO, Aldrich TK, Nagel RI et al - Accuracy of pulse oximetry
Demographics, such as age, gender or race do not influence in sickle cell disease. Am J Respir Crit Care Med, 1999;159:
SpO2 - SaO2 ratio 13. In blacks, SpO2 below 95% reflects SaO2 447-451.
below90%, while in Caucasians this same SpO2 value is 92% 6. 12. Barker SJ, Tremper KK, Hyatt J et al - Effects of methemoglobin
Normal SpO 2 - SaO 2 gap values vary between plus or minus on pulse oximetry and mixed venous oximetry. Anesthesiology,
1989;70:112-117.
3% to 5% 6 .
13. Saber W, McCarthy K, Schilz R - Limitations of pulse oximetry.
In anesthesia, and especially in intensive care, SpO 2 is used Chest, 2000;118:184S.
to identify changes in ventilator settings. Assuming normal
SpO 2 - SaO 2 gap values, lower SpO 2 values between 92%
and 94% are used to prevent SaO 2 going below 90%, which
corresponds to mild hypoxemia 3-6 . However, in critically ill RESUMEN
patients under mechanical ventilation, lower SpO 2 limit Helayel PE, Oliveira Filho GR, Marcon L, Pederneiras FH, Nico-
lodi MA, Pederneiras SG - Gradiente SpO2 - SaO2 Durante Ven-
should be 96% to avoid hypoxemia during changes in ventila-
tilación Mecánica en Anestesia y Terapia Intensiva
tor settings 2 .
In our study, 95.28% of patients showed SpO 2 - SaO 2 gap
Justificativas y Objetivos - La saturación periférica de la
values within mismatching limits, that is, two standard devia- oxihemoglobina (SpO2) es frecuentemente utilizada para guiar
tions above and below the mean difference, but 4.72% alteraciones del régimen ventilatorio. Valores de SpO2 iguales
showed excessively high values. In such cases, if the lowest o superiores a 96% son necesarios para garantizar saturación
Revista Brasileira de Anestesiologia 309
Vol. 51, Nº 4, Julho - Agosto, 2001
HELAYEL, OLIVEIRA FILHO, MARCON ET AL
arterial de la oxihemoglobina (SaO2) superiores a 90%, en Resultados - Fueron analizadas 228 muestras. La diferencia
pacientes de terapia intensiva. Este estudio tuvo por objetivo entre los valores de SpO2 y SaO2 varió entre -7,10% y 15,20%,
determinar concordancia entre valores de SpO2 y SaO2 y siendo la diferencia media igual a -0,20% ± 2,02%. SpO2-SaO2
delimitar la menor SpO2 asociada con valores de SaO2 iguales mayores que 4,04% (dos desvíos padrones de la diferencia)
o superiores a 90%. ocurrieron en 4,72% de las muestras. La determinación gráfica
Método - Fueron incluidos prospectivamente 120 pacientes de la SpO2, mínima para garantizar la SaO2 arriba de 90%,
adultos, de ambos sexos, sometidos a anestesia general con mostró que solamente valores de SpO2 iguales o superiores a
ventilación mecánica o en tratamiento intensivo. Muestras de 99% no se asociaron con la ocurrencia de ningún valor de SaO2
sangre arterial fueron colectadas por punción arterial o por inferior a 90%.
aspiración de línea arterial, utilizando técnica anaeróbia, en Conclusiones - Aun cuando la diferencia entre los valores de
jeringas heparinizadas. Las muestras fueron analizadas SpO2 y SaO2 se hallan localizados entre más y menos 5% en
inmediatamente después de la colecta. La SpO2 fue medida por 97% de los pares analizados, solamente valores arriba de 99%
oxímetro de pulso durante la colecta, en el indicador de la mano excluyeron pacientes con SaO2 menor que 90%.
contra-lateral, utilizando la onda dicrótica de pulso arterial
como parámetro de adecuación.
310 Revista Brasileira de Anestesiologia
Vol. 51, Nº 4, Julho - Agosto, 2001
Você também pode gostar
- Modelo de Laudo Autismo em PDF AtdocxDocumento3 páginasModelo de Laudo Autismo em PDF AtdocxProfessora Claudia100% (2)
- Solos Não Saturados 20015 PDFDocumento792 páginasSolos Não Saturados 20015 PDFJonattan OliveiraAinda não há avaliações
- Animais PeçonhentosDocumento5 páginasAnimais PeçonhentosElielson SousaAinda não há avaliações
- Formulário de Pediatria, 3a Ed.Documento100 páginasFormulário de Pediatria, 3a Ed.Ângela Maresch75% (8)
- Aula Avaliacao Antropometrica Do IdosoDocumento22 páginasAula Avaliacao Antropometrica Do IdosoViviane MacedoAinda não há avaliações
- E Book Ferramentas para Manutencao Industrial Volume 1Documento84 páginasE Book Ferramentas para Manutencao Industrial Volume 1JoséAinda não há avaliações
- 5 Aspiracao de Vias AereasDocumento37 páginas5 Aspiracao de Vias AereasDeysiane Macêdo100% (1)
- EletrostaticaDocumento45 páginasEletrostaticatatz_angel79% (24)
- Lei de Gauss - TeoriaDocumento6 páginasLei de Gauss - TeoriaFelipe CarvalhoAinda não há avaliações
- Le Ca A09 J GR 260508Documento16 páginasLe Ca A09 J GR 260508Buba ZettAinda não há avaliações
- Industria Da Seca e Familias Desagregadas Artigo 2012Documento32 páginasIndustria Da Seca e Familias Desagregadas Artigo 2012JoséAinda não há avaliações
- Sonoff Schmatic PDFDocumento2 páginasSonoff Schmatic PDFoscar.diciomma8446Ainda não há avaliações
- Lafer Em618 PDF Apostila Engrenagens 4Documento25 páginasLafer Em618 PDF Apostila Engrenagens 4flaviafernandes21Ainda não há avaliações
- Dimensionamento de Ar CondicionadoDocumento9 páginasDimensionamento de Ar CondicionadoGylnara CarvalhêdoAinda não há avaliações
- 4 - Potência Elétrica e Circ TrifásicosDocumento12 páginas4 - Potência Elétrica e Circ TrifásicosJoséAinda não há avaliações
- Informática - Autocad 3DDocumento370 páginasInformática - Autocad 3DExcelly100% (2)
- Informática - Autocad 3DDocumento370 páginasInformática - Autocad 3DExcelly100% (2)
- Aterramento 1Documento24 páginasAterramento 1JoséAinda não há avaliações
- Apostila MCU PDFDocumento115 páginasApostila MCU PDFVanildo SilvaAinda não há avaliações
- O Espa Co Euclidiano R: Cap Itulo 1Documento21 páginasO Espa Co Euclidiano R: Cap Itulo 1Apocalipse10Ainda não há avaliações
- Siloc PU 55 Cola para Parabrisa de CarroDocumento2 páginasSiloc PU 55 Cola para Parabrisa de CarroJoséAinda não há avaliações
- Bomba Grundfos CRI 3 - 10Documento2 páginasBomba Grundfos CRI 3 - 10JoséAinda não há avaliações
- Automação PneumáticaDocumento73 páginasAutomação PneumáticaCarlosSilva100% (1)
- Notas FourierDocumento36 páginasNotas FourierJoséAinda não há avaliações
- Capitulo 2Documento88 páginasCapitulo 2Luciano LejesAinda não há avaliações
- 354Documento39 páginas354Augusto GoulartAinda não há avaliações
- Apostila de Portugues Estruturado PDFDocumento7 páginasApostila de Portugues Estruturado PDFJoséAinda não há avaliações
- Limites Indeterminados e Regras de L' HospitalDocumento9 páginasLimites Indeterminados e Regras de L' HospitalRil SilvaAinda não há avaliações
- Apostila de Portugues EstruturadoDocumento26 páginasApostila de Portugues EstruturadoJoséAinda não há avaliações
- Localizador de Defeitos - DicasDocumento11 páginasLocalizador de Defeitos - DicasRafael FávaroAinda não há avaliações
- Lei de BeerDocumento4 páginasLei de BeerAnaileCostaAinda não há avaliações
- Curva FETs PDFDocumento16 páginasCurva FETs PDFJoséAinda não há avaliações
- Dados Tecnicos ECG - 6 EcafixDocumento1 páginaDados Tecnicos ECG - 6 EcafixJoséAinda não há avaliações
- Equações Diferenciais Ordinárias e Introdução Aos Sistemas DinâmicosDocumento100 páginasEquações Diferenciais Ordinárias e Introdução Aos Sistemas DinâmicosJoséAinda não há avaliações
- CAROLINA2009Documento80 páginasCAROLINA2009Romário LuizAinda não há avaliações
- Plano de Cuidados PTADocumento14 páginasPlano de Cuidados PTAlilianas803100% (1)
- SLAN - PosterDocumento12 páginasSLAN - PosterLuis AnunciacaoAinda não há avaliações
- Etiologia DoençaperioDocumento57 páginasEtiologia DoençaperioLuiza FerrazAinda não há avaliações
- Avaliação FuncionalDocumento27 páginasAvaliação FuncionalDanielly Rios PlusSizeAinda não há avaliações
- Cronograma de Hof Semi PresencialDocumento4 páginasCronograma de Hof Semi PresencialAmanda Costa RodriguesAinda não há avaliações
- Nanofarmacologia Na Modulação Celular e OncologiaDocumento4 páginasNanofarmacologia Na Modulação Celular e OncologiaWendreane VitóriaAinda não há avaliações
- Doenças Infecciosas de Interesse VeterinárioDocumento77 páginasDoenças Infecciosas de Interesse VeterinárioVictóriaAinda não há avaliações
- Diagnostico Por Imagem em Caes e GatosDocumento16 páginasDiagnostico Por Imagem em Caes e GatosPriscilla SouzaAinda não há avaliações
- Ciências 9º Ano Atividade Da SemanaDocumento3 páginasCiências 9º Ano Atividade Da Semanamario dalmolinAinda não há avaliações
- Teoria Da MassagemDocumento26 páginasTeoria Da Massagemcaianap100% (1)
- Exame OftalmoDocumento3 páginasExame OftalmoUnifimesAinda não há avaliações
- GP de URO - Seção 4Documento36 páginasGP de URO - Seção 4AvhaPaixão100% (1)
- Resum ÃoDocumento12 páginasResum ÃoGuileneAidarCeronAinda não há avaliações
- Reuxen Ant InflamatorioDocumento5 páginasReuxen Ant Inflamatoriojoão_robalo_5Ainda não há avaliações
- Caso Clinico-Cardiopatia AcianóticaDocumento63 páginasCaso Clinico-Cardiopatia AcianóticaevertonAinda não há avaliações
- NomofobiaDocumento3 páginasNomofobiageisa rochaAinda não há avaliações
- TRE SE Dentistas CredenciadosDocumento44 páginasTRE SE Dentistas CredenciadosflavioAinda não há avaliações
- UntitledDocumento19 páginasUntitledcamilo carlos-eduardo166hotmaiI.comAinda não há avaliações
- Revista Aromaterapet Jun 2022Documento18 páginasRevista Aromaterapet Jun 2022teacherletyAinda não há avaliações
- Resultado: 99 MG/DL: GlicoseDocumento4 páginasResultado: 99 MG/DL: GlicoseMariluci MarquesAinda não há avaliações
- Estudo de Caso Kelen 0804Documento19 páginasEstudo de Caso Kelen 0804Karla ToledoAinda não há avaliações
- Uso de Drogas Deccorentes Transtornos MentaisDocumento14 páginasUso de Drogas Deccorentes Transtornos MentaisDiogo alvesAinda não há avaliações
- EstomiasDocumento6 páginasEstomiasAna AliceAinda não há avaliações
- Guia Medico VersaoDocumento183 páginasGuia Medico VersaoGustavo LimaAinda não há avaliações