Você também pode gostar
- O Papel Do Farmacêutico Na Cicatrização De FeridasNo EverandO Papel Do Farmacêutico Na Cicatrização De FeridasAinda não há avaliações
- Técnica de Microagulhamento Associado Ao Ácido TranexâmicoDocumento13 páginasTécnica de Microagulhamento Associado Ao Ácido TranexâmicoBeatriz CristinaAinda não há avaliações
- MD Codes: Uma abordagem metodológica para preenchimento facialDocumento13 páginasMD Codes: Uma abordagem metodológica para preenchimento facialcesargradellaAinda não há avaliações
- Apostila Aulao M.A 2206Documento94 páginasApostila Aulao M.A 2206Amora AmadaAinda não há avaliações
- Protocolo 1 Rejuvenescimento Fototipo 1 A 5 PDFDocumento17 páginasProtocolo 1 Rejuvenescimento Fototipo 1 A 5 PDFErik BrooksAinda não há avaliações
- Análise da dentição decíduaDocumento20 páginasAnálise da dentição decíduaLuciana RagiAinda não há avaliações
- Preços Botulift, Ácido Hialurônico, Microagulhamento e Linha EstéticaDocumento1 páginaPreços Botulift, Ácido Hialurônico, Microagulhamento e Linha EstéticaPAULO TELLESAinda não há avaliações
- Utilização Dos Bioestimuladores de Colágeno Na Harmonização OrofacialDocumento18 páginasUtilização Dos Bioestimuladores de Colágeno Na Harmonização OrofacialLucelia Alves SoaresAinda não há avaliações
- Final - Lets HOF - PreenchimentoFacial - Ebook - CópiaDocumento72 páginasFinal - Lets HOF - PreenchimentoFacial - Ebook - Cópiacamilumba2017Ainda não há avaliações
- Protocolo Rejuvenescimento Fototipo 6 PDFDocumento23 páginasProtocolo Rejuvenescimento Fototipo 6 PDFErik BrooksAinda não há avaliações
- Termo Peeling de FenolDocumento2 páginasTermo Peeling de FenolAndressa GreinAinda não há avaliações
- Pressuriderm Harmony Filler CADocumento2 páginasPressuriderm Harmony Filler CAJoaquim Zed100% (1)
- Curso de Hidra Gloss LipsDocumento12 páginasCurso de Hidra Gloss LipsDaniel WeissAinda não há avaliações
- Ácido MandélicoDocumento2 páginasÁcido MandélicoFrancisco AugustoAinda não há avaliações
- MICROAGULHAMENTODocumento12 páginasMICROAGULHAMENTOGabrielAinda não há avaliações
- Angela Microbotox-PHD Novo LogoDocumento39 páginasAngela Microbotox-PHD Novo LogoCamila CarvalhoAinda não há avaliações
- Ellansé® - 2019 PDFDocumento34 páginasEllansé® - 2019 PDFAlline BoliariniAinda não há avaliações
- Apostila - AnatomiaDocumento19 páginasApostila - AnatomiaDra Mariana Cioffi100% (1)
- Cicatricure É Bom Mesmo para Rugas e EstriasDocumento3 páginasCicatricure É Bom Mesmo para Rugas e EstriasClaudio Gomes Silva LeiteAinda não há avaliações
- Micropigmentação Capilar - Apostila 1Documento10 páginasMicropigmentação Capilar - Apostila 1Ytallo FaustinoAinda não há avaliações
- Sagah 13 LaserterapiaDocumento19 páginasSagah 13 LaserterapialohAinda não há avaliações
- Ultrassom - EstéticaDocumento17 páginasUltrassom - EstéticaLAURA NUNES SANTANAAinda não há avaliações
- Protocolo ACNE SPEC ProfissionalDocumento2 páginasProtocolo ACNE SPEC ProfissionalDayana Lima CarvalhoAinda não há avaliações
- LUMINECENSE v4Documento2 páginasLUMINECENSE v4Maria José PradoAinda não há avaliações
- Hyaluronic pen para tratamentos estéticosDocumento50 páginasHyaluronic pen para tratamentos estéticosSrta AraújoAinda não há avaliações
- Consentimento informado para procedimentos com Hyaluron PenDocumento1 páginaConsentimento informado para procedimentos com Hyaluron PenLuzia AlvesAinda não há avaliações
- Guia Tecnico DigitalDocumento136 páginasGuia Tecnico DigitalJoao Victor Souza100% (1)
- Anatomia da pele e tratamentos com ácido hialurônicoDocumento18 páginasAnatomia da pele e tratamentos com ácido hialurônicoJoici Santos0% (1)
- Protocolos Faciais La VertuanDocumento23 páginasProtocolos Faciais La VertuanLarissa Alves100% (2)
- CURSO MICRO MAKEUP BB GLOWDocumento4 páginasCURSO MICRO MAKEUP BB GLOWMaria CarolinaAinda não há avaliações
- Acido FiticoDocumento4 páginasAcido FiticoIsteuria Cristina100% (1)
- Curso de camuflagem de estrias e cicatrizesDocumento31 páginasCurso de camuflagem de estrias e cicatrizesCras UrucuiaAinda não há avaliações
- Ativos Dermatológicos e Hidratação CorporalDocumento98 páginasAtivos Dermatológicos e Hidratação CorporalCamyla FernandezAinda não há avaliações
- v1 Laser No Rejuvenescimento Facial PDFDocumento8 páginasv1 Laser No Rejuvenescimento Facial PDFvini_tbAinda não há avaliações
- Livro MAP 2.0Documento110 páginasLivro MAP 2.0Camila Steinbach100% (1)
- Protocolo de peeling com AHA's e LED para clareamento e renovação celularDocumento7 páginasProtocolo de peeling com AHA's e LED para clareamento e renovação celularMarina MolinariAinda não há avaliações
- Técnica de MicropunturaDocumento9 páginasTécnica de MicropunturaNataliaAinda não há avaliações
- Belotero Range DigitalDocumento2 páginasBelotero Range DigitalArcelino FariasAinda não há avaliações
- Anatomia e fisiologia da peleDocumento40 páginasAnatomia e fisiologia da peleMaria Gabriela Alves de SouzaAinda não há avaliações
- Peeling Químico Sem Medo e de Forma Segura: Como Fazer e Deixar A Pele Da Sua PacienteDocumento70 páginasPeeling Químico Sem Medo e de Forma Segura: Como Fazer e Deixar A Pele Da Sua PacienteKarine NascimentoAinda não há avaliações
- Enviando Por Email Protocolo Clareamento Master Estética Natural BoticaDocumento6 páginasEnviando Por Email Protocolo Clareamento Master Estética Natural Boticairis silva silvaAinda não há avaliações
- Catalogo SamanaDocumento57 páginasCatalogo SamanaPaula Guima100% (1)
- Cuidados Pós PeelingDocumento1 páginaCuidados Pós Peelingcelia.regina.meneghiniAinda não há avaliações
- Fatores de crescimento manipulação feridasDocumento1 páginaFatores de crescimento manipulação feridasNany BellumatAinda não há avaliações
- Ebook MESOBOTOXDocumento3 páginasEbook MESOBOTOXFrancieli Torquato CostaBeber50% (2)
- Vertical Co2 Fractional Laser ManualDocumento16 páginasVertical Co2 Fractional Laser ManualAnthoni PeixotoAinda não há avaliações
- Manejo dermatológico para diferentes tipos de peleDocumento16 páginasManejo dermatológico para diferentes tipos de peleIvan Pontes AguiarAinda não há avaliações
- (Aula 1) Intensivao 2023 - CompressedDocumento115 páginas(Aula 1) Intensivao 2023 - CompressedKarina LeipeltAinda não há avaliações
- BiolumitáDocumento2 páginasBiolumitáEdersson NaitzAinda não há avaliações
- Peeling QuímicoDocumento9 páginasPeeling QuímicoFrancielson CarvalhoAinda não há avaliações
- Como Tratar o Envelhecimento CutâneoDocumento60 páginasComo Tratar o Envelhecimento CutâneoAna Paula Pereira Cunha100% (1)
- Laser Tera PiaDocumento52 páginasLaser Tera PiaLuh TeixeiraAinda não há avaliações
- Slides Intradermoterapia INAESP 2022 Rev PDFDocumento197 páginasSlides Intradermoterapia INAESP 2022 Rev PDFJúlia Peçanha PinhoAinda não há avaliações
- Lâmina - NutricolinDocumento2 páginasLâmina - NutricolinPriscila Cordeiro100% (2)
- Camuflagem de estrias: técnicas, riscos e como funcionaDocumento52 páginasCamuflagem de estrias: técnicas, riscos e como funcionaMonicaAinda não há avaliações
- Acido L-Polilatico CorporalDocumento57 páginasAcido L-Polilatico CorporalGlória Cabral DocenteAinda não há avaliações
- Dermaplaning passo a passo guiaDocumento9 páginasDermaplaning passo a passo guiaDany PadyAinda não há avaliações
- Captura de Tela 2023-07-23 À(s) 21.53.59Documento137 páginasCaptura de Tela 2023-07-23 À(s) 21.53.59Juliete santosAinda não há avaliações
- Depilação A Laser e LedDocumento39 páginasDepilação A Laser e LedvsmfisioterapeutaAinda não há avaliações
- Microagulhamento Estudo Experimental e Classificacao Da Injuria ProvocadaDocumento5 páginasMicroagulhamento Estudo Experimental e Classificacao Da Injuria ProvocadaMarina Molinari100% (1)
- Exame cito-oncológico e cito-hormonalDocumento1 páginaExame cito-oncológico e cito-hormonalCamila VazAinda não há avaliações
- Aula 42 - Autacoides e AntagonistasDocumento46 páginasAula 42 - Autacoides e AntagonistasMarcos SoaresAinda não há avaliações
- Ética e pandemiasDocumento19 páginasÉtica e pandemiasDaniel BorgesAinda não há avaliações
- 6 A Desparasitação Interna Do CãoDocumento1 página6 A Desparasitação Interna Do CãoSara FerreiraAinda não há avaliações
- Aula 2 Relação Parasito-HospedeiroDocumento37 páginasAula 2 Relação Parasito-HospedeiroAriana AlvesAinda não há avaliações
- Livro - Unico Biotec-1 PDFDocumento196 páginasLivro - Unico Biotec-1 PDFMaione LinsAinda não há avaliações
- Livro ColunaDocumento326 páginasLivro ColunaMilene Eloisa100% (1)
- Meridiano Estômago BaçoDocumento3 páginasMeridiano Estômago BaçoHARE KRISHNAAinda não há avaliações
- Patologia Circulatória: Distúrbios da CirculaçãoDocumento46 páginasPatologia Circulatória: Distúrbios da CirculaçãoGabriel Messias100% (1)
- Manual Tas TatDocumento122 páginasManual Tas TatromeonederlandsAinda não há avaliações
- Bioquímica - Metabolismo Da BilirrubinaDocumento18 páginasBioquímica - Metabolismo Da Bilirrubinasuporte telessaudeAinda não há avaliações
- Passivo agressivo; avalie se é seu casoDocumento6 páginasPassivo agressivo; avalie se é seu casovkarmo100% (1)
- Estudo Dirigido AnatomiaDocumento10 páginasEstudo Dirigido Anatomiaivan andradeAinda não há avaliações
- 98 - 2021 Diretrizes Do Exercício Profissional Do Fisioterapeuta No Âmbito HospitalarDocumento10 páginas98 - 2021 Diretrizes Do Exercício Profissional Do Fisioterapeuta No Âmbito HospitalarKamila OliveiraAinda não há avaliações
- Câncer de Próstata: Anatomia, Epidemiologia e Fatores de RiscoDocumento8 páginasCâncer de Próstata: Anatomia, Epidemiologia e Fatores de RiscoBells MarquesAinda não há avaliações
- Documentação de Saberes Indígenas Vol. VDocumento164 páginasDocumentação de Saberes Indígenas Vol. VJoana SilvaAinda não há avaliações
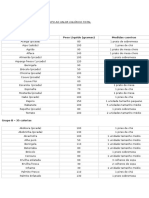
- Classificação de alimentos por valor calóricoDocumento4 páginasClassificação de alimentos por valor calóricoMariannabalinhas100% (1)
- (Da Dor Ao Alívio) Ebook 3Documento16 páginas(Da Dor Ao Alívio) Ebook 3kaoliveAinda não há avaliações
- Aula 14 - Agentes Anti-Inflamatórios Não Esteroides IDocumento96 páginasAula 14 - Agentes Anti-Inflamatórios Não Esteroides IAlvaro Galdos50% (2)
- Teste de Coombs direto avalia anticorpos ligados a hemáciasDocumento4 páginasTeste de Coombs direto avalia anticorpos ligados a hemáciasAnderson RodriguesAinda não há avaliações
- Meridiano e Pontos Do VGDocumento5 páginasMeridiano e Pontos Do VGsaulowAinda não há avaliações
- Doenças do Sistema ExcretorDocumento2 páginasDoenças do Sistema ExcretorMirelly Carvalho AlcântaraAinda não há avaliações
- Dermato 2 PDFDocumento18 páginasDermato 2 PDFBRUNO MONTEIROAinda não há avaliações
- 1.cm-Cir - Síndrome IctéricaDocumento6 páginas1.cm-Cir - Síndrome IctéricaGuilherme SousaAinda não há avaliações
- Análise de distribuição de frequência de colesterol totalDocumento22 páginasAnálise de distribuição de frequência de colesterol totalJuan MonteiroAinda não há avaliações
- Aula 02Documento20 páginasAula 02LeandroNobreAinda não há avaliações
- Gripe Aviária - Wikipédia, A Enciclopédia LivreDocumento21 páginasGripe Aviária - Wikipédia, A Enciclopédia LivreThiago FernandesAinda não há avaliações
- Demônios e suas atuaçõesDocumento9 páginasDemônios e suas atuaçõesDROGA FAMILY14% (7)
- Curso especialização geriatriaDocumento62 páginasCurso especialização geriatriaGabrielle RoccheAinda não há avaliações
- Farmácia Bioquímica - Versão BDocumento20 páginasFarmácia Bioquímica - Versão BnadiellesiqueiraAinda não há avaliações