Você também pode gostar
- Fisiopatologia Das ArritmiasDocumento51 páginasFisiopatologia Das ArritmiasTeresaSM19Ainda não há avaliações
- Tese MEGI Filipa LagesDocumento143 páginasTese MEGI Filipa LagesTeresaSM19Ainda não há avaliações
- Farmacologia Da DMDocumento82 páginasFarmacologia Da DMTeresaSM19Ainda não há avaliações
- Saúde Pública Baseada em Evidências - Ross CDocumento1 páginaSaúde Pública Baseada em Evidências - Ross CTeresaSM19Ainda não há avaliações
- Farmacologia Da DIIDocumento22 páginasFarmacologia Da DIITeresaSM19Ainda não há avaliações
- Competencias Gerenciais No Ambito Dos Institutos Federais de EducacaoDocumento103 páginasCompetencias Gerenciais No Ambito Dos Institutos Federais de EducacaoTeresaSM19Ainda não há avaliações
- Anti ArrítmicosDocumento7 páginasAnti ArrítmicosTeresaSM19Ainda não há avaliações
- Fármacos Usados Na Doença Isquémica Coronária e Insuficiência CardíacaDocumento11 páginasFármacos Usados Na Doença Isquémica Coronária e Insuficiência CardíacaTeresaSM19Ainda não há avaliações
- Sistema Vestibular: Córtex Tálamo Hipotálamo MeningesDocumento1 páginaSistema Vestibular: Córtex Tálamo Hipotálamo MeningesTeresaSM19Ainda não há avaliações
- AnticoagulantesDocumento4 páginasAnticoagulantesTeresaSM19Ainda não há avaliações
- Fármacos DiabetesDocumento12 páginasFármacos DiabetesTeresaSM19100% (1)
- Sebenta Neuroanatomia Fucking God Volume 1 - 1 EdiçãoDocumento96 páginasSebenta Neuroanatomia Fucking God Volume 1 - 1 EdiçãoTeresaSM19Ainda não há avaliações
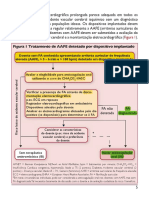
- Guidelines para FA Do Caso 3Documento10 páginasGuidelines para FA Do Caso 3TeresaSM19Ainda não há avaliações
- Anti HTPDocumento6 páginasAnti HTPTeresaSM19Ainda não há avaliações
- Sebenta Neuroanatomia Fucking God Volume 1 - 1 EdiçãoDocumento96 páginasSebenta Neuroanatomia Fucking God Volume 1 - 1 EdiçãoTeresaSM19Ainda não há avaliações
- The Nervous System - Peripheral Atlas (UNLOCKED) (FML) PDFDocumento267 páginasThe Nervous System - Peripheral Atlas (UNLOCKED) (FML) PDFTeresaSM19Ainda não há avaliações
- Farmacodinâmica - ConceitosDocumento5 páginasFarmacodinâmica - ConceitosTeresaSM19Ainda não há avaliações
- Sistematização de Angiologia - Artéria, Veias e Linfáticos (Wired - FML) PDFDocumento76 páginasSistematização de Angiologia - Artéria, Veias e Linfáticos (Wired - FML) PDFTeresaSM19Ainda não há avaliações
- 2 - Destino Dos Folhetos GerminativosDocumento2 páginas2 - Destino Dos Folhetos GerminativosTeresaSM19Ainda não há avaliações
- 1 - GametogéneseDocumento2 páginas1 - GametogéneseTeresaSM19Ainda não há avaliações
- Smooth Dissection #ÉpoarrasoDocumento436 páginasSmooth Dissection #ÉpoarrasoTeresaSM19Ainda não há avaliações
- Sebenta Neuroanatomia Fucking God Volume 1 - 2 Edic - A - O-2Documento102 páginasSebenta Neuroanatomia Fucking God Volume 1 - 2 Edic - A - O-2TeresaSM19Ainda não há avaliações
- Sebenta Neuroanatomia Fucking God Volume 1 - 2 Edic - A - O-2Documento102 páginasSebenta Neuroanatomia Fucking God Volume 1 - 2 Edic - A - O-2TeresaSM19Ainda não há avaliações
- Neuroanatomia - Rita Luz PDFDocumento212 páginasNeuroanatomia - Rita Luz PDFTeresaSM19Ainda não há avaliações
- Sistema Nervoso Autónomo 3EDDocumento20 páginasSistema Nervoso Autónomo 3EDTeresaSM19Ainda não há avaliações
- Plexos - Anaisa AfonsoDocumento24 páginasPlexos - Anaisa AfonsoTeresaSM19Ainda não há avaliações
- Pares Cranianos - Anaisa Afonso PDFDocumento26 páginasPares Cranianos - Anaisa Afonso PDFTeresaSM19Ainda não há avaliações
- Reflexoes Do Poeta Os LusiadasDocumento36 páginasReflexoes Do Poeta Os LusiadasTeresaSM19100% (1)
- Imagens Rouviere CompiladasDocumento226 páginasImagens Rouviere CompiladasAnonymous mEU3GDIQDAinda não há avaliações
- FARMACOVIGILÂNCIADocumento10 páginasFARMACOVIGILÂNCIADayanna CunhaAinda não há avaliações
- Doenças Prevalentes Da InfânciaDocumento29 páginasDoenças Prevalentes Da InfânciaLiane LeitãoAinda não há avaliações
- Guia Qualificacao Cds 2022Documento34 páginasGuia Qualificacao Cds 2022Leônido Silva100% (1)
- Sinopse Do Case - Diabetes GestacionalDocumento6 páginasSinopse Do Case - Diabetes GestacionalLuciana AlvarezAinda não há avaliações
- Mapa Mental - Primeiros SocorrosDocumento65 páginasMapa Mental - Primeiros SocorrosMarcelo SurlemontAinda não há avaliações
- Homeopatia Indicações DeaazDocumento327 páginasHomeopatia Indicações DeaazPaula Alves OshiroAinda não há avaliações
- Aula Crise HipertensivaDocumento20 páginasAula Crise Hipertensivakleberleilsson100% (1)
- Distrofia Muscular de DuchenneDocumento10 páginasDistrofia Muscular de DuchenneDuda MeloAinda não há avaliações
- Semiologia RenalDocumento6 páginasSemiologia RenalPedro CardosoAinda não há avaliações
- Bula 0000000037331Documento25 páginasBula 0000000037331Coordenacaofarmacia hrlAinda não há avaliações
- Trabalho de Ciencias Doenças Respiratorias e Alergias AlimentaresDocumento16 páginasTrabalho de Ciencias Doenças Respiratorias e Alergias AlimentaresMonique Vieira Botelho MachadoAinda não há avaliações
- Prevenção e Controle Da Dor em OdontologiaDocumento3 páginasPrevenção e Controle Da Dor em OdontologiaLara CarnioAinda não há avaliações
- Prevenção CombinadaDocumento2 páginasPrevenção CombinadaMaria Clara De AngeliAinda não há avaliações
- Leucemia Mieloide CronicaDocumento15 páginasLeucemia Mieloide CronicaSabrina CarvalhoAinda não há avaliações
- ToracocenteseDocumento3 páginasToracocenteseCarlos AntônioAinda não há avaliações
- Doenças DesmielinizantesDocumento59 páginasDoenças DesmielinizantesTalita De Almeida100% (1)
- Parasitologia - HelmintosDocumento44 páginasParasitologia - Helmintosluiz4sAinda não há avaliações
- Prescrição Internação EnfermariaDocumento1 páginaPrescrição Internação EnfermariardsmedpaAinda não há avaliações
- FSQ+-+Fibromyalgia+Survey+Questionnaire+ (I Ndice+de+Dor+Generalizada+++SSS+Versa O+questiona Rio)Documento3 páginasFSQ+-+Fibromyalgia+Survey+Questionnaire+ (I Ndice+de+Dor+Generalizada+++SSS+Versa O+questiona Rio)Rafael RochaAinda não há avaliações
- Apostila - PancreatiteDocumento2 páginasApostila - PancreatiteThiago OliveiraAinda não há avaliações
- Programa de HiperdiaDocumento2 páginasPrograma de HiperdiaFernanda CoelhoAinda não há avaliações
- Ae Sec Bio12 Questao Aula 3Documento3 páginasAe Sec Bio12 Questao Aula 3Ana RITAAinda não há avaliações
- Calendário Vacinal Da Gestante-DeSCOMPLICA ENFERMAGEMDocumento12 páginasCalendário Vacinal Da Gestante-DeSCOMPLICA ENFERMAGEMClaudiely Lenz0% (1)
- Ciclo Fungos CULTURA FUNGICA PARA DERMATOFITOS E LEVEDURASDocumento2 páginasCiclo Fungos CULTURA FUNGICA PARA DERMATOFITOS E LEVEDURASraphaeltnvAinda não há avaliações
- Herpes ZosterDocumento6 páginasHerpes ZosterStephany AvelarAinda não há avaliações
- Aula TraqueostomiaDocumento18 páginasAula TraqueostomiaVanessaAinda não há avaliações
- E Book Gratuito Resistência À Insulina PDFDocumento19 páginasE Book Gratuito Resistência À Insulina PDFKarine OsternoAinda não há avaliações
- Meningite ViralDocumento16 páginasMeningite ViralGustavo LuisAinda não há avaliações
- Projeto Todos Contra A DengueDocumento28 páginasProjeto Todos Contra A DengueFernanda CunhaAinda não há avaliações
- Ficha Registos VORTEXDocumento1 páginaFicha Registos VORTEXSandrina CrespoAinda não há avaliações