Você também pode gostar
- Resumo Seguranca e Saude Do TrabalhoDocumento165 páginasResumo Seguranca e Saude Do Trabalhoklaudinha88100% (5)
- Relato de Caso - Matricídio, Seguido de Canibalismo e AutomutilaçãoDocumento4 páginasRelato de Caso - Matricídio, Seguido de Canibalismo e AutomutilaçãofrancopessiniAinda não há avaliações
- Cartilha SuicídioDocumento2 páginasCartilha SuicídioVagner AméricoAinda não há avaliações
- Filicídio e Psicose Relato de Dois CasosDocumento3 páginasFilicídio e Psicose Relato de Dois CasosRone lino da SilvaAinda não há avaliações
- Comportamento Suicida Entre AdolescentesDocumento9 páginasComportamento Suicida Entre AdolescentesAlexandra ValériaAinda não há avaliações
- Cartilha Setembro Amarelo Obra 618Documento2 páginasCartilha Setembro Amarelo Obra 618Ana OliveiraAinda não há avaliações
- Obsessions of Infanticide and Imminent Psychosis: A.H. Chapman, Miriam Chapman-Santana, Simone A. TeixeiraDocumento4 páginasObsessions of Infanticide and Imminent Psychosis: A.H. Chapman, Miriam Chapman-Santana, Simone A. TeixeiraJOSÉ DAVID SALCEDO CASTROAinda não há avaliações
- Risco Suicidário em JovensDocumento13 páginasRisco Suicidário em JovensCrislaine FernandesAinda não há avaliações
- Setembro Amarelo 2022Documento20 páginasSetembro Amarelo 2022Luan da Silva Inácio LuanAinda não há avaliações
- A Atuação Do Enfermeiro Com A Pessoa em Situação de SuicídioDocumento7 páginasA Atuação Do Enfermeiro Com A Pessoa em Situação de SuicídioClaudio Gruber MannAinda não há avaliações
- Risco de Suicídio em Jovens Com Transtornos de Ansiedade - Estudo de Base PopulacionalDocumento4 páginasRisco de Suicídio em Jovens Com Transtornos de Ansiedade - Estudo de Base PopulacionalsekillaAinda não há avaliações
- Língua Portuguesa: Glícia CamposDocumento8 páginasLíngua Portuguesa: Glícia Camposthaylanascimento846Ainda não há avaliações
- Suicidio TanatologiaDocumento3 páginasSuicidio TanatologiaPe. Genivaldo dos SantosAinda não há avaliações
- Suicídio Como Tema de Reflexão BioéticaDocumento6 páginasSuicídio Como Tema de Reflexão BioéticaCaio SilvaAinda não há avaliações
- ArtigoDocumento8 páginasArtigoDébora Scheneider HoffmeisterAinda não há avaliações
- PACCIOLLA, Aureliano. Cognitivismo - Existencial - e - SuicidioDocumento25 páginasPACCIOLLA, Aureliano. Cognitivismo - Existencial - e - SuicidioMarcio Junior100% (1)
- Prev Suicídio CRP RNDocumento32 páginasPrev Suicídio CRP RNRodrigo Costa de OliveiraAinda não há avaliações
- SUICÍDIODocumento17 páginasSUICÍDIOAnonymous C3HopKi6mIAinda não há avaliações
- Baptista 2017 Case ReportDocumento4 páginasBaptista 2017 Case ReportNatammyAinda não há avaliações
- Membership Areaaula20completa20sem20marcadores - PdfresDocumento30 páginasMembership Areaaula20completa20sem20marcadores - PdfresVerônica V.Ainda não há avaliações
- Identificando Comportamentos e Ideações: Um Olhar Ampliado Sobre Os Fatores de RiscoDocumento28 páginasIdentificando Comportamentos e Ideações: Um Olhar Ampliado Sobre Os Fatores de RiscoCarol SouzaAinda não há avaliações
- AutolesaoDocumento14 páginasAutolesaoAnne BritoAinda não há avaliações
- 01 A Incidencia Do Suicidio Na Adolescencia - 1265466023Documento6 páginas01 A Incidencia Do Suicidio Na Adolescencia - 1265466023profisisgonzaga24Ainda não há avaliações
- Neuronios SuicidioDocumento4 páginasNeuronios SuicidiolucasfneuropsiAinda não há avaliações
- SetembroDocumento14 páginasSetembroAnna RakelAinda não há avaliações
- TCC - Suicídio Na Adolescência-1Documento22 páginasTCC - Suicídio Na Adolescência-1Bianca CurveloAinda não há avaliações
- Prevenção Ao SuicidioDocumento24 páginasPrevenção Ao SuicidioJéssica DanúziaAinda não há avaliações
- Setembro Amarelo EstadualDocumento20 páginasSetembro Amarelo EstadualDesirê BuenoAinda não há avaliações
- Cópia de Trabalho Da Prof CarlaDocumento11 páginasCópia de Trabalho Da Prof CarlaSandra MuandaAinda não há avaliações
- Automutilacao 2018Documento12 páginasAutomutilacao 2018Antonio Augusto Pinto JuniorAinda não há avaliações
- Pacientes em Risco de SuicidioDocumento10 páginasPacientes em Risco de SuicidioJhulyane CunhaAinda não há avaliações
- OPP Prevenir SuicidioDocumento20 páginasOPP Prevenir SuicidioÂngeloOliveiraAinda não há avaliações
- 9290-Texto Do Artigo-43819-1-10-20190901Documento14 páginas9290-Texto Do Artigo-43819-1-10-20190901Hérico MacielAinda não há avaliações
- Suicidio SCDocumento12 páginasSuicidio SCAna Paula Gomes de ArmasAinda não há avaliações
- Guia Intersetorial de Prevenção Do Comportamento Suicida em Crianças e AdolescentesDocumento19 páginasGuia Intersetorial de Prevenção Do Comportamento Suicida em Crianças e AdolescentesLarissaAinda não há avaliações
- 8-Saúde Da Criança e Adolescente Parte 2Documento36 páginas8-Saúde Da Criança e Adolescente Parte 2Douglas HammesAinda não há avaliações
- Guia Intersetorial de Prevencao Do Comportamento Suicida em Criancas e Adolescentes 2019Documento36 páginasGuia Intersetorial de Prevencao Do Comportamento Suicida em Criancas e Adolescentes 2019Vi KekaAinda não há avaliações
- COELHO Et Al. 2009 Suicidio de Internos em Um Hospital de Custodia e TratamentoDocumento5 páginasCOELHO Et Al. 2009 Suicidio de Internos em Um Hospital de Custodia e TratamentoJ M EAinda não há avaliações
- SETEMBRO AMARELO Miriam GorenderDocumento10 páginasSETEMBRO AMARELO Miriam GorenderAdriana MesquitaAinda não há avaliações
- v14 09 Ago 2021Documento6 páginasv14 09 Ago 2021Bruna MoraisAinda não há avaliações
- Suicídio para EscolaDocumento4 páginasSuicídio para EscolaAssistencia Social Sec SaúdeAinda não há avaliações
- Detecção Do Risco de Suicidio Nos Serviços de Emergência PsiquiátricaDocumento9 páginasDetecção Do Risco de Suicidio Nos Serviços de Emergência PsiquiátricaCGMann2009Ainda não há avaliações
- DNB Vol31 No4 413Documento8 páginasDNB Vol31 No4 413Hiago Teixeira DamacianoAinda não há avaliações
- Setembro Amarelo Suicidio Orientando A PrevençãoDocumento16 páginasSetembro Amarelo Suicidio Orientando A PrevençãoCPSSTAinda não há avaliações
- Níveis de Ideação Suicida em Jovens AdultosDocumento10 páginasNíveis de Ideação Suicida em Jovens AdultosLucas LiberatoAinda não há avaliações
- SuicidioDocumento25 páginasSuicidioFabricia Nogueira De CamargoAinda não há avaliações
- WerlangDocumento8 páginasWerlangivy_intheryeAinda não há avaliações
- Manejo em Emergencia Do Paciente SuicidaDocumento6 páginasManejo em Emergencia Do Paciente SuicidaJulianaAinda não há avaliações
- Emergncias Peditricas Emergncias Psiquitricas em Crianas e AdolescentesDocumento12 páginasEmergncias Peditricas Emergncias Psiquitricas em Crianas e Adolescentesamanda-fontenelesAinda não há avaliações
- Impacto Do Estresse de Minoria em Pessoas TransDocumento13 páginasImpacto Do Estresse de Minoria em Pessoas Transawnjiminx xAinda não há avaliações
- DownloadDocumento4 páginasDownloadIza silvaAinda não há avaliações
- Caso Cutting-Artigo-2 Com ReferenciasDocumento5 páginasCaso Cutting-Artigo-2 Com ReferenciasEliezer GrilloAinda não há avaliações
- Trabalho Acadêmico de TanatologiaDocumento15 páginasTrabalho Acadêmico de TanatologiaJocéli Grobério de OliveiraAinda não há avaliações
- 501 1397 1 PBDocumento19 páginas501 1397 1 PBCrislaine Do PradoAinda não há avaliações
- 2018 14 Setembro Amarelo Vamos Falar Sobre Suicã - DioDocumento26 páginas2018 14 Setembro Amarelo Vamos Falar Sobre Suicã - DioVanessa X LíncolisAinda não há avaliações
- 24505-Texto Do Trabalho-94823-1-10-20210428Documento8 páginas24505-Texto Do Trabalho-94823-1-10-20210428MafaldaGomesAinda não há avaliações
- Palestra Imesrsao Das EmocoesDocumento13 páginasPalestra Imesrsao Das Emocoeswanderlucia100% (1)
- Suicidio Uma Epidemia SilenciosaDocumento31 páginasSuicidio Uma Epidemia SilenciosaSueli RufineAinda não há avaliações
- Adolescência, Suicídio, Mutilação e BullyingDocumento74 páginasAdolescência, Suicídio, Mutilação e BullyingAndreiaCristinaGaglianoAinda não há avaliações
- Considerações sobre o suicídio no Brasil: Teoria e estudo de casosNo EverandConsiderações sobre o suicídio no Brasil: Teoria e estudo de casosAinda não há avaliações
- Informativo Tematico 2023 Atualizado 1121Documento288 páginasInformativo Tematico 2023 Atualizado 1121elmoAinda não há avaliações
- 17 Professor de MatemáticaDocumento12 páginas17 Professor de MatemáticaWilson SantosAinda não há avaliações
- Técnicas Anestésicas Da MaxilaDocumento14 páginasTécnicas Anestésicas Da MaxilaSileimar LopesAinda não há avaliações
- Artigo - Ingluviotomia em CalopsitaDocumento8 páginasArtigo - Ingluviotomia em CalopsitaFlavia da RosaAinda não há avaliações
- Empreendedorismo Governamental e Novas Lideranças No Setor Público.Documento5 páginasEmpreendedorismo Governamental e Novas Lideranças No Setor Público.Weyland Ewerton Leila CarvalhoAinda não há avaliações
- Ultrassom PulmonarDocumento51 páginasUltrassom PulmonarPaulo AguiarAinda não há avaliações
- Massagem Relaxante - Conceitos e TécnicasDocumento48 páginasMassagem Relaxante - Conceitos e TécnicasJu ArquivosestudarAinda não há avaliações
- Treinamento para Operador de BetoneiraDocumento2 páginasTreinamento para Operador de BetoneiraBC CUNHAAinda não há avaliações
- Vasculites Medcurso CompletoDocumento5 páginasVasculites Medcurso Completocamila mendesAinda não há avaliações
- Aula 2 Dr. Ricardo Guimaraes Intro Fundacao Hospital de Olhos Curso Profess Ores Dislexia de LeituraDocumento22 páginasAula 2 Dr. Ricardo Guimaraes Intro Fundacao Hospital de Olhos Curso Profess Ores Dislexia de LeituraRicardo Guimaraes100% (1)
- Metodos de EsterilizacaoDocumento1 páginaMetodos de EsterilizacaoAdalbertoAinda não há avaliações
- A Pessoa Estomizada: Análise Das Práticas Educativas de EnfermagemDocumento8 páginasA Pessoa Estomizada: Análise Das Práticas Educativas de EnfermagemPablo CandidoAinda não há avaliações
- 2004848368-Mayara Pereira de SouzaDocumento6 páginas2004848368-Mayara Pereira de SouzaMayara SouzaAinda não há avaliações
- Classificação Dos ParasitasDocumento1 páginaClassificação Dos ParasitasAna SophiaAinda não há avaliações
- Aula 13 Traumatologia I Acao MecanicaDocumento75 páginasAula 13 Traumatologia I Acao MecanicaBrado AfricanoAinda não há avaliações
- RubéolaDocumento2 páginasRubéolaTeo SilvaAinda não há avaliações
- Validação de Transporte de HemocomponentesDocumento39 páginasValidação de Transporte de HemocomponentesYARAAinda não há avaliações
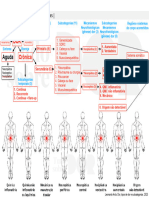
- Organograma Dor, Tipos de Dor e SubcategoriasDocumento1 páginaOrganograma Dor, Tipos de Dor e SubcategoriasIvan W LossAinda não há avaliações
- Relatorio de Visita Tecnica EdilmaDocumento7 páginasRelatorio de Visita Tecnica EdilmaEdilma SilvaAinda não há avaliações
- Meridianos de Passagem - LoDocumento15 páginasMeridianos de Passagem - LoandreaguirredoamaralAinda não há avaliações
- 52 Nota para Mural 116 Orientacaoo Acerca Da Avaliacao de Desempenho Profissional Intelectual EplDocumento16 páginas52 Nota para Mural 116 Orientacaoo Acerca Da Avaliacao de Desempenho Profissional Intelectual EplPaulo SergioAinda não há avaliações
- Zimduck - o Remédio Natural Que Nos Protege de Infecções e Aumenta A ImunidadeDocumento2 páginasZimduck - o Remédio Natural Que Nos Protege de Infecções e Aumenta A ImunidadeOlivarAinda não há avaliações
- 04 - Aula Formas Farmacêuticas Sólidas Pós, Grânulos, Cásulas e ComprimidosDocumento33 páginas04 - Aula Formas Farmacêuticas Sólidas Pós, Grânulos, Cásulas e ComprimidosRichardson AlbuquerqueAinda não há avaliações
- CFM Na Pandemia de Covid-19Documento55 páginasCFM Na Pandemia de Covid-19Conceição Lemes100% (1)
- 1 - Manual de Atua - o Do Promotor de Justi - A Na Defesa Da Pessoa Idosa PDFDocumento62 páginas1 - Manual de Atua - o Do Promotor de Justi - A Na Defesa Da Pessoa Idosa PDFLetízia CunhaAinda não há avaliações
- Transtorno Alimentar Na Infancia Nem Cid e Nem DSM ComentariosDocumento7 páginasTranstorno Alimentar Na Infancia Nem Cid e Nem DSM ComentariosCaroline OliveiraAinda não há avaliações
- Tecnologias Do Corpo Uma Antropologia Das MedicinaDocumento3 páginasTecnologias Do Corpo Uma Antropologia Das MedicinaAna Lúcia AlbanoAinda não há avaliações
- Fispq Fastac 100 PT 10.09.2019Documento15 páginasFispq Fastac 100 PT 10.09.2019LeonardoAinda não há avaliações
- Caderno Especial DengueDocumento10 páginasCaderno Especial DengueAndryo CardosoAinda não há avaliações