Você também pode gostar
- O Mapa para Acumular 1 Milão de MilhasDocumento88 páginasO Mapa para Acumular 1 Milão de MilhasGERUSA RIBEIRO91% (11)
- Pentest em Redes de Computadore - Royce DavisDocumento418 páginasPentest em Redes de Computadore - Royce Davisdiegobastos88Ainda não há avaliações
- Simulador de RobôDocumento26 páginasSimulador de RobôLeonardo Figliolino de OliveiraAinda não há avaliações
- Profetas Maiores Josue Brandao Apostila MedioDocumento25 páginasProfetas Maiores Josue Brandao Apostila MedioEMERSON ROCHA100% (1)
- Alfa4port Solucoes Livro Fichas-3Documento8 páginasAlfa4port Solucoes Livro Fichas-3Sérgio Mélice83% (12)
- Moreira, 2010Documento10 páginasMoreira, 2010DanielBCAinda não há avaliações
- MEEM - Padronização e Instruções de Uso PDFDocumento12 páginasMEEM - Padronização e Instruções de Uso PDFJanaina Albuquerque Marques PintoAinda não há avaliações
- Texto 03 - EpsDocumento12 páginasTexto 03 - EpsCINTHYA DANIELLE DOS REIS LEALAinda não há avaliações
- Ficha Exame NeurológicoDocumento1 páginaFicha Exame NeurológicoCaio WilggnerAinda não há avaliações
- Manual de Cardiologia 2016 Rev Out 2016Documento18 páginasManual de Cardiologia 2016 Rev Out 2016marimedvet0Ainda não há avaliações
- Modelación Competitiva Carga InternaDocumento129 páginasModelación Competitiva Carga InternaJOEL MUÑOZAinda não há avaliações
- DownloadDocumento8 páginasDownloadMahdi HosseiniAinda não há avaliações
- 3 Revista - Educacao - Continuada - Vol - 12 - No - 2 - 2014Documento100 páginas3 Revista - Educacao - Continuada - Vol - 12 - No - 2 - 2014Taty CavalliniAinda não há avaliações
- Características Antropométricas, Composição Corporal e Somatotipo Por Esportes. Dados de Referência Do CAR Sant Cugat, 1989-2013Documento8 páginasCaracterísticas Antropométricas, Composição Corporal e Somatotipo Por Esportes. Dados de Referência Do CAR Sant Cugat, 1989-2013Éden SiqueiraAinda não há avaliações
- A Relacao Da Involucao Psicomotora Com o Numero de Quedas em Idosas Praticantes e Nao Praticantes de Exercicio Fisico RegularDocumento133 páginasA Relacao Da Involucao Psicomotora Com o Numero de Quedas em Idosas Praticantes e Nao Praticantes de Exercicio Fisico RegularEmaMateus100% (2)
- Meem Padronizacao e Instrucoes de UsoDocumento12 páginasMeem Padronizacao e Instrucoes de UsoJorge Leonardo Cardoso AssumpçãoAinda não há avaliações
- Demência - EEGDocumento7 páginasDemência - EEGGabi SeabraAinda não há avaliações
- A Utilização Do Cavalo em Paciente Com Transtorno Do Espectro Autista Uma Revisão IntegrativaDocumento10 páginasA Utilização Do Cavalo em Paciente Com Transtorno Do Espectro Autista Uma Revisão IntegrativaLuiza StacowskiAinda não há avaliações
- Escalas de AvaliaçãoDocumento147 páginasEscalas de AvaliaçãoMichelle SINIMBÚAinda não há avaliações
- Bem-Estar Psicológico eDocumento10 páginasBem-Estar Psicológico eJosemeire L. S. StatellaAinda não há avaliações
- Anaclaudia 02. Mar.2021 LuaDocumento15 páginasAnaclaudia 02. Mar.2021 LuaGeorgeKielingAinda não há avaliações
- (20211200-PT) Fisioterapia Desportiva 06 43357Documento24 páginas(20211200-PT) Fisioterapia Desportiva 06 43357Felipe Smith TeixeiraAinda não há avaliações
- Com 26 321 23 Cronograma Geral Ed. 1.321.23 Versao Final DOE Atualizado 1Documento12 páginasCom 26 321 23 Cronograma Geral Ed. 1.321.23 Versao Final DOE Atualizado 1Mr. Mime MobileAinda não há avaliações
- Pré Projeto Do TCC (Atualizado Quase100%)Documento29 páginasPré Projeto Do TCC (Atualizado Quase100%)Jonas PessoaAinda não há avaliações
- Habilidades Viso-Perceptuais e Motoras Na Síndrome de AspergerDocumento141 páginasHabilidades Viso-Perceptuais e Motoras Na Síndrome de AspergerDenise Lima100% (1)
- Trabalho de Conclusão de Curso I - Taise TomioDocumento42 páginasTrabalho de Conclusão de Curso I - Taise TomioAdriele Feléx LimaAinda não há avaliações
- Sistema Cardiorespiratório e FisioterapiaDocumento1 páginaSistema Cardiorespiratório e Fisioterapiaomeu papelcriativoAinda não há avaliações
- Silo - Tips Fisioterapiab R A S I LDocumento456 páginasSilo - Tips Fisioterapiab R A S I Ljozeilton.dbAinda não há avaliações
- FICHAMENTODocumento3 páginasFICHAMENTOPaulo CorreiaAinda não há avaliações
- Pré Projeto Do TCCDocumento28 páginasPré Projeto Do TCCJonas PessoaAinda não há avaliações
- Saude Mental Trabalho CartilhaDocumento15 páginasSaude Mental Trabalho CartilhaJuliano Lauria88% (8)
- 1 PBDocumento78 páginas1 PBThays W. OliveiraAinda não há avaliações
- Silo - Tips Analise Das Escalas Desenvolvidas para Avaliar A Funao Motora de Pacientes Com Paralisia CerebralDocumento72 páginasSilo - Tips Analise Das Escalas Desenvolvidas para Avaliar A Funao Motora de Pacientes Com Paralisia CerebralDaniela NevesAinda não há avaliações
- Barbosa-Silva2016 en PTDocumento6 páginasBarbosa-Silva2016 en PTJúlia BenckeAinda não há avaliações
- Revista Portuguesa Ciências Do Desporto: Artigos de Investigação (Research Papers)Documento168 páginasRevista Portuguesa Ciências Do Desporto: Artigos de Investigação (Research Papers)Thiago MonteiroAinda não há avaliações
- GG v8n3Documento64 páginasGG v8n3Anderson FerroBemAinda não há avaliações
- Revista FisiobrasilDocumento136 páginasRevista FisiobrasilGessyPb0% (1)
- Determinantes Sociais e Economicos Da Saude MentalDocumento6 páginasDeterminantes Sociais e Economicos Da Saude MentalIsabelly AntunesAinda não há avaliações
- Documentação Necessária para Abertura de Processos para Medicamentos Do Comportamento Agressivo No Transtorno Do Espectro Do AutismoDocumento3 páginasDocumentação Necessária para Abertura de Processos para Medicamentos Do Comportamento Agressivo No Transtorno Do Espectro Do AutismoSimoneAinda não há avaliações
- Relatório de Fisiologia (Aferição de Pressão)Documento10 páginasRelatório de Fisiologia (Aferição de Pressão)Vitor SilvaAinda não há avaliações
- Ponte 2017Documento7 páginasPonte 2017smmendoncaAinda não há avaliações
- Doenças Neurodegenerativas e o ExercícioDocumento21 páginasDoenças Neurodegenerativas e o ExercícioBernardo LopesAinda não há avaliações
- Valores de Referencia de Forca de Preensao Manual para HomensDocumento5 páginasValores de Referencia de Forca de Preensao Manual para HomensAcilino PortelaAinda não há avaliações
- Fofito - 25 - Set - Dez 2007Documento100 páginasFofito - 25 - Set - Dez 2007salvadoorjrAinda não há avaliações
- Proteção ArticularDocumento16 páginasProteção ArticularBruna AmorimAinda não há avaliações
- (20231100-PT) Medicina DesportivaDocumento36 páginas(20231100-PT) Medicina DesportivaManuel CasanovaAinda não há avaliações
- Monografia RosaDocumento45 páginasMonografia RosaArmando António InácioAinda não há avaliações
- Cronograma PMDocumento29 páginasCronograma PMdigrau014Ainda não há avaliações
- Revista Cbpaemh 2009Documento122 páginasRevista Cbpaemh 2009rodjelisalviAinda não há avaliações
- MetodologiaDocumento1 páginaMetodologiajeronimoAinda não há avaliações
- MetodologiaDocumento1 páginaMetodologiajeronimoAinda não há avaliações
- CP 140311Documento144 páginasCP 140311Elis HaraAinda não há avaliações
- Acupressão para A AnsiedadeDocumento1 páginaAcupressão para A AnsiedadeAlan Douglas CordeiroAinda não há avaliações
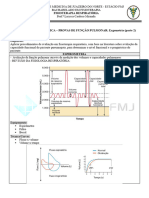
- Prática PulmonarDocumento3 páginasPrática Pulmonarrenamasso22Ainda não há avaliações
- Práticas Integrativas e Complementares Como Recurso Da SM Na ABDocumento9 páginasPráticas Integrativas e Complementares Como Recurso Da SM Na ABIsabela DuqueAinda não há avaliações
- Escalas de Avaliação Motora para Indivíduos Com ParalisiaDocumento14 páginasEscalas de Avaliação Motora para Indivíduos Com ParalisiaRita Alexandra PinzónAinda não há avaliações
- Respostas Fisiológicas Ao Exercício Físico em Lesados MedularesDocumento9 páginasRespostas Fisiológicas Ao Exercício Físico em Lesados MedularesAugusto FerreiraAinda não há avaliações
- Eficácia Da Ventosaterapia Na Prática EsportivaDocumento20 páginasEficácia Da Ventosaterapia Na Prática EsportivaDanielle OliveiraAinda não há avaliações
- 1517 8692 Rbme 20 04 00276Documento5 páginas1517 8692 Rbme 20 04 00276Luciano CamargosAinda não há avaliações
- Utilização Da Acupuntura Na Doença de AlzheimerDocumento9 páginasUtilização Da Acupuntura Na Doença de AlzheimerSchasta JensenAinda não há avaliações
- Artigoleo 2Documento2 páginasArtigoleo 2Aff CaxiasAinda não há avaliações
- Praticantes de Uma Modalidade Desportiva Federada Têm Melhor Coordenação Motora em Relação A Crianças Que Não As Pratiquem?Documento28 páginasPraticantes de Uma Modalidade Desportiva Federada Têm Melhor Coordenação Motora em Relação A Crianças Que Não As Pratiquem?Nuno Santos (TheSexyGarlic)Ainda não há avaliações
- Fisioterapia Brasilv 15 N 2 Marabr 2014Documento85 páginasFisioterapia Brasilv 15 N 2 Marabr 2014Rafael RochaAinda não há avaliações
- Dor psíquica, dor corporal: uma abordagem multidisciplinarNo EverandDor psíquica, dor corporal: uma abordagem multidisciplinarAinda não há avaliações
- Gelson Santos CVDocumento1 páginaGelson Santos CVYBC CHAGVVAAinda não há avaliações
- A Busca Do Jesus HistóricoDocumento8 páginasA Busca Do Jesus Históricopedro_2009Ainda não há avaliações
- TecnicasDocumento6 páginasTecnicascmutti2010Ainda não há avaliações
- 3 - Emendas ÓpticasDocumento31 páginas3 - Emendas ÓpticasVinicius SantosAinda não há avaliações
- Cadeias Produtivas Do Agronegócio Ii: Ronei Tiago SteinDocumento21 páginasCadeias Produtivas Do Agronegócio Ii: Ronei Tiago Steingustavojhonattan99Ainda não há avaliações
- Oficina o Ator PresenteDocumento1 páginaOficina o Ator PresenteMário CôrtesAinda não há avaliações
- Three Little PigsDocumento3 páginasThree Little PigsAmanda MalinoskiAinda não há avaliações
- Suelen Vollerthun Dos Santos MachadoDocumento25 páginasSuelen Vollerthun Dos Santos MachadoCentral Smart InformaticaAinda não há avaliações
- NomeDocumento6 páginasNomeKelry VasconcelosAinda não há avaliações
- Novas Ferramentas de Corte e SoluçõesDocumento64 páginasNovas Ferramentas de Corte e SoluçõesGustavo GiattiAinda não há avaliações
- Exercicios Parte I - ESMI 24Documento2 páginasExercicios Parte I - ESMI 24Jamilo Dos SantosAinda não há avaliações
- Prova Integrada 2 - 1º Semestre 2022Documento47 páginasProva Integrada 2 - 1º Semestre 2022FELIPE EMANUEL BASNIAK DA SILVA (A)Ainda não há avaliações
- Paper Grupo de FisioterapiaDocumento2 páginasPaper Grupo de FisioterapiaElisabete de BarrosAinda não há avaliações
- A Cosmologia Bíblica, Conforme o Senhor, em Sua Misericórdia, Nos Revelou PDF 4Documento40 páginasA Cosmologia Bíblica, Conforme o Senhor, em Sua Misericórdia, Nos Revelou PDF 4José Carlos R. OliveiraAinda não há avaliações
- A GravuraDocumento28 páginasA GravuraJaime João ManuelAinda não há avaliações
- Teste de EstanqueidadeDocumento26 páginasTeste de EstanqueidadeRonaldo Alves Oliveira100% (1)
- Concurso Público - Um GUIA COMPLETO Até Chegar À AprovaçãoDocumento20 páginasConcurso Público - Um GUIA COMPLETO Até Chegar À AprovaçãoBACX CONTABILAinda não há avaliações
- Manual Do UsuárioDocumento172 páginasManual Do UsuárioLuiz100% (1)
- Diversidade e o Campo Da Educação - Relatos de PesquisaDocumento198 páginasDiversidade e o Campo Da Educação - Relatos de PesquisaAntonioSardAinda não há avaliações
- P05 - Planta de Construção TérreoDocumento1 páginaP05 - Planta de Construção TérreoSamuel Nogueira da SilvaAinda não há avaliações
- Manso e HumildeDocumento3 páginasManso e HumildeCamila RamosAinda não há avaliações
- A Matemática Da Villa Ideal - Colin RoweDocumento22 páginasA Matemática Da Villa Ideal - Colin RoweSthefany BeatrizAinda não há avaliações
- O Que É Adolescencia GlauDocumento18 páginasO Que É Adolescencia GlauGlaucielen CristinaAinda não há avaliações
- Denver Tec 100Documento3 páginasDenver Tec 100logus10Ainda não há avaliações
- Charges de Infancia - Escolarização Da Infância - Nas Charges de Francesco TonucciDocumento19 páginasCharges de Infancia - Escolarização Da Infância - Nas Charges de Francesco TonucciKeelzinhaaaAinda não há avaliações