Você também pode gostar
- Resumo & Guia De Estudo - Planeta Vazio: O Declínio Chocante Da População MundialNo EverandResumo & Guia De Estudo - Planeta Vazio: O Declínio Chocante Da População MundialNota: 1 de 5 estrelas1/5 (1)
- Breve História Da Saúde Pública No BrasilDocumento8 páginasBreve História Da Saúde Pública No BrasilFernando Machado100% (1)
- Modulo IntrodutorioDocumento21 páginasModulo IntrodutorioJuniorGleyssonCruzAinda não há avaliações
- Thais Martins - Trabalho de SociologiaDocumento2 páginasThais Martins - Trabalho de SociologiaGpkaiAinda não há avaliações
- Figueira Et Al 2020 Povos Indigenas e A Pandemia Covid-19 No Brasil - Um Genocídio AnunciadoDocumento16 páginasFigueira Et Al 2020 Povos Indigenas e A Pandemia Covid-19 No Brasil - Um Genocídio Anunciadoadrielensilva.7Ainda não há avaliações
- A Abolição e A Manutenção Das Injustiças - A Luta Dos Negros Na Primeira República Brasileira.Documento10 páginasA Abolição e A Manutenção Das Injustiças - A Luta Dos Negros Na Primeira República Brasileira.Lucca IgnácioAinda não há avaliações
- HOCHMAN, G. SILVA, R. Campanhas Públicas, Populações (Quase) Invisíveis Endemias Rurais e Indígenas Na Saúde Pública BrasileiraDocumento22 páginasHOCHMAN, G. SILVA, R. Campanhas Públicas, Populações (Quase) Invisíveis Endemias Rurais e Indígenas Na Saúde Pública BrasileiraRoger CodatirumAinda não há avaliações
- Jane Beltrão-Povos Indígenas, Saúde e DitaduraDocumento10 páginasJane Beltrão-Povos Indígenas, Saúde e DitaduraEwerton_TumaAinda não há avaliações
- Estudo Sobre Indígenas Infectados Por IstDocumento24 páginasEstudo Sobre Indígenas Infectados Por IstAlvimcaAinda não há avaliações
- Quem Manipula Os Povos Indigenas Contra o Desenvolvimento Do Brasil Autores Lorenzo Carrasco e Silvia Palacios PDFDocumento16 páginasQuem Manipula Os Povos Indigenas Contra o Desenvolvimento Do Brasil Autores Lorenzo Carrasco e Silvia Palacios PDFNatan AlvesAinda não há avaliações
- La Dansarina: A Gripe Espanhola e o Cotidiano Na Cidade Do Rio de JaneiroDocumento21 páginasLa Dansarina: A Gripe Espanhola e o Cotidiano Na Cidade Do Rio de JaneiroRafaelAinda não há avaliações
- Resenhas de Teoria Do Direito IIDocumento5 páginasResenhas de Teoria Do Direito IIBigSmoke OtakuAinda não há avaliações
- Populaçoes Rndígenas No Século Descobrimento: E Problemas: AS DO DO AspectosDocumento21 páginasPopulaçoes Rndígenas No Século Descobrimento: E Problemas: AS DO DO AspectosLarissa Esther de Freitas BrandãoAinda não há avaliações
- Povos Indígenas Brasileiros em Tempos Pandêmicos Crise Viral e Governamental A Serviço Do Assimilacionismo CulturalDocumento21 páginasPovos Indígenas Brasileiros em Tempos Pandêmicos Crise Viral e Governamental A Serviço Do Assimilacionismo CulturalDaniel SouzaAinda não há avaliações
- História Da Saúde Pública No Brasil: Solange BertoziDocumento12 páginasHistória Da Saúde Pública No Brasil: Solange BertoziCarla GracieteAinda não há avaliações
- A Demografia No Antigo RegimeDocumento4 páginasA Demografia No Antigo RegimeMário MontesAinda não há avaliações
- Ebook Redação - Repertorio - IndigenasDocumento17 páginasEbook Redação - Repertorio - Indigenaslourajulia2Ainda não há avaliações
- Resenha Do Livro Morte Na Floresta, de Aparecida Vilaça, Publicado em 2020.Documento4 páginasResenha Do Livro Morte Na Floresta, de Aparecida Vilaça, Publicado em 2020.monalisatreveriAinda não há avaliações
- Resenhas de Teoria Do Direito IIDocumento8 páginasResenhas de Teoria Do Direito IIBigSmoke OtakuAinda não há avaliações
- Atividade 1 - História Do BrasilDocumento3 páginasAtividade 1 - História Do Brasilfernanda stocklerAinda não há avaliações
- Trabalho de Matematica Do Matheus 2 AnoDocumento4 páginasTrabalho de Matematica Do Matheus 2 Anojulio CézarAinda não há avaliações
- 161550-Texto Do Artigo-386362-1-10-20191225Documento21 páginas161550-Texto Do Artigo-386362-1-10-20191225Fabíola KonsalikAinda não há avaliações
- A História Da Tuberculose e Do TuberculosoDocumento246 páginasA História Da Tuberculose e Do TuberculosoLuciana Hastenreiter CavanellasAinda não há avaliações
- Documento 1Documento1 páginaDocumento 1Harley MoraisAinda não há avaliações
- Cláudia Fernandes - Up202106689Documento1 páginaCláudia Fernandes - Up202106689Claudia FernandesAinda não há avaliações
- Saúde Dos Povos Indígenas Reflexões Sobre Antropologia Participativa. LANGDON Esther J. GARNELO Luiza.Documento13 páginasSaúde Dos Povos Indígenas Reflexões Sobre Antropologia Participativa. LANGDON Esther J. GARNELO Luiza.tetebarddalAinda não há avaliações
- 1 PBDocumento9 páginas1 PBNicole SilvaAinda não há avaliações
- A Censura e Outros Limites - EXP COMPLETODocumento292 páginasA Censura e Outros Limites - EXP COMPLETOCaio B. BarreiraAinda não há avaliações
- 7bdain Borges - Inchado Feio - compLEMENTARDocumento28 páginas7bdain Borges - Inchado Feio - compLEMENTARGabriel MontesAinda não há avaliações
- Tema 2 Pensamento VincularDocumento9 páginasTema 2 Pensamento VincularMagda ElaneAinda não há avaliações
- 3-A Morte Por Jejuy Entre Os Guarani Do Sudoeste Brasileiro - Miguel Vicente FotiDocumento28 páginas3-A Morte Por Jejuy Entre Os Guarani Do Sudoeste Brasileiro - Miguel Vicente FotiAlani BenvenuttiAinda não há avaliações
- Ficha - Nossa GenteDocumento7 páginasFicha - Nossa GenteDyllan SoaresAinda não há avaliações
- Admin, ART 600 BJDDocumento10 páginasAdmin, ART 600 BJDPaulo TadeuAinda não há avaliações
- Projeto de Pesquisa Apresentado Ao CursoDocumento10 páginasProjeto de Pesquisa Apresentado Ao CursoFernanda PerrúAinda não há avaliações
- A História Das Pandemias Contada Por Erico Veríssimo e Pedro NavaDocumento20 páginasA História Das Pandemias Contada Por Erico Veríssimo e Pedro NavaPablo QueirozAinda não há avaliações
- Atividade 1 - História Do Brasil CorreçãoDocumento3 páginasAtividade 1 - História Do Brasil Correçãofernanda stocklerAinda não há avaliações
- Ve Erica Ell Etal 2020Documento2 páginasVe Erica Ell Etal 2020Gabriel AbreuAinda não há avaliações
- "Não Existe Pecado Do Lado de Baixo Do Equador", Mas Enfermidades...Documento5 páginas"Não Existe Pecado Do Lado de Baixo Do Equador", Mas Enfermidades...Nilvanete de LimaAinda não há avaliações
- Tempos Autoritários, Crimes e Danos À Saúde deDocumento16 páginasTempos Autoritários, Crimes e Danos À Saúde deTallyta SuennyAinda não há avaliações
- Redação Nota 1000 - Da Escrita A CorreçãoDocumento3 páginasRedação Nota 1000 - Da Escrita A CorreçãoNeusa GotoAinda não há avaliações
- 2020-04 Revista-Ilaese 07Documento76 páginas2020-04 Revista-Ilaese 07Leandro AntunesAinda não há avaliações
- Raça DegeneraçãoDocumento28 páginasRaça DegeneraçãoAna CristinaAinda não há avaliações
- Nteha11 Ficha1 Res PDFDocumento2 páginasNteha11 Ficha1 Res PDFHelena ReisAinda não há avaliações
- Ganjodossantos, 2 - 1918 HISTÓRIA E A PANDEMIADocumento16 páginasGanjodossantos, 2 - 1918 HISTÓRIA E A PANDEMIASufismo, O Caminho Místico Do IslamAinda não há avaliações
- Aula 4 O Brasil Do SertãoDocumento35 páginasAula 4 O Brasil Do SertãoDIOGO SILVA MANOELAinda não há avaliações
- História-Semana 08 - T4Documento10 páginasHistória-Semana 08 - T4MARCELO REGIUS GOMES BASTOSAinda não há avaliações
- Memrias Da Dor o Patrimnio Sensvel Da PandemiaDocumento20 páginasMemrias Da Dor o Patrimnio Sensvel Da PandemiaVíctor Veríssimo GuimarãesAinda não há avaliações
- Atividades Questão IndígenaDocumento3 páginasAtividades Questão IndígenaBreno Augusto Alves Pereira RosaAinda não há avaliações
- Geografia - MigraçãoDocumento2 páginasGeografia - MigraçãoMarcella MagaldiAinda não há avaliações
- A População Da Europa Nos Séculos XVII e XVIII - Crises e Crescimento 11 AnoDocumento12 páginasA População Da Europa Nos Séculos XVII e XVIII - Crises e Crescimento 11 AnoAna Isabel RibeiroAinda não há avaliações
- Aprovar Ano05 Livro26 008Documento1 páginaAprovar Ano05 Livro26 008vestibaprovarueaAinda não há avaliações
- Desigualdades RaciaisDocumento9 páginasDesigualdades RaciaisElias FernandesAinda não há avaliações
- Lista de Exercícios - População 3Documento22 páginasLista de Exercícios - População 3Miguel GuerraAinda não há avaliações
- Aula Referente Ao Dia 23 de Junho. GeografiaDocumento3 páginasAula Referente Ao Dia 23 de Junho. GeografiaLucasAinda não há avaliações
- Vrds,+artigo Final +Revista+do+Gelne - 15 06 Revisado - Diagramado - 86 101Documento16 páginasVrds,+artigo Final +Revista+do+Gelne - 15 06 Revisado - Diagramado - 86 101Stefany FerrazAinda não há avaliações
- Prova Processo Seletivo Indigena UFSM 2020Documento16 páginasProva Processo Seletivo Indigena UFSM 2020vitorjochimsAinda não há avaliações
- Atividade - 11-08-2020 - População Mundial - 2 Série - GeografiaDocumento3 páginasAtividade - 11-08-2020 - População Mundial - 2 Série - GeografiaRobson Pontes0% (1)
- Povos Pré-Colombianos Na América ContemporâneaDocumento7 páginasPovos Pré-Colombianos Na América ContemporâneaCalil CavalcanteAinda não há avaliações
- Emigração e Sanitarismo - Porto e Brasil No Seculo XIXDocumento26 páginasEmigração e Sanitarismo - Porto e Brasil No Seculo XIXJorge Fernandes AlvesAinda não há avaliações
- Declaracao de Concordancia Grupo de PesquisaDocumento1 páginaDeclaracao de Concordancia Grupo de PesquisaIsnara Pereira IvoAinda não há avaliações
- Diretrizes para Dissertação Profhistória UesbDocumento19 páginasDiretrizes para Dissertação Profhistória UesbIsnara Pereira IvoAinda não há avaliações
- SELEÇÃODocumento1 páginaSELEÇÃOIsnara Pereira IvoAinda não há avaliações
- Projeto Uma Historia Dos Sertoes No BrasilDocumento17 páginasProjeto Uma Historia Dos Sertoes No BrasilIsnara Pereira IvoAinda não há avaliações
- Normas AutoresDocumento28 páginasNormas AutoresIsnara Pereira IvoAinda não há avaliações
- Normas para Elaboração Projeto de Pesquisa ProfhistoriaDocumento3 páginasNormas para Elaboração Projeto de Pesquisa ProfhistoriaIsnara Pereira IvoAinda não há avaliações
- Regimento Geral Do ProfHistóriaDocumento13 páginasRegimento Geral Do ProfHistóriaIsnara Pereira IvoAinda não há avaliações
- Extensao 2022 Isnara P IvoDocumento12 páginasExtensao 2022 Isnara P IvoIsnara Pereira IvoAinda não há avaliações
- Resolucao Consepe - Regimento ProfHistoriaDocumento19 páginasResolucao Consepe - Regimento ProfHistoriaIsnara Pereira IvoAinda não há avaliações
- Quantitativo de Orientandos-Orientadores 2022.2 (Divididos Por Linha de Pesquisa)Documento1 páginaQuantitativo de Orientandos-Orientadores 2022.2 (Divididos Por Linha de Pesquisa)Isnara Pereira IvoAinda não há avaliações
- Proposta Evento - MestiçagensDocumento2 páginasProposta Evento - MestiçagensIsnara Pereira IvoAinda não há avaliações
- Genero Honor y Esclavitud La DiferenciaDocumento26 páginasGenero Honor y Esclavitud La DiferenciaIsnara Pereira IvoAinda não há avaliações
- Cro No GramaDocumento1 páginaCro No GramaIsnara Pereira IvoAinda não há avaliações
- Informacao para Processo 00043591310Documento1 páginaInformacao para Processo 00043591310Isnara Pereira IvoAinda não há avaliações
- Parecer Tecnico 00043506969Documento2 páginasParecer Tecnico 00043506969Isnara Pereira IvoAinda não há avaliações
- Atividade 4 SoraiaDocumento2 páginasAtividade 4 SoraiaIsnara Pereira IvoAinda não há avaliações
- 14 Outras Solicitações Ficha de MatrículaDocumento1 página14 Outras Solicitações Ficha de MatrículaIsnara Pereira IvoAinda não há avaliações
- Cartagena de Indias e Salvador Uma AnaliDocumento32 páginasCartagena de Indias e Salvador Uma AnaliIsnara Pereira IvoAinda não há avaliações
- Escravidão, Mestiçagem e Histórias ComparadasDocumento353 páginasEscravidão, Mestiçagem e Histórias ComparadasIsnara Pereira IvoAinda não há avaliações
- Edital Novas Disciplinas 2022Documento2 páginasEdital Novas Disciplinas 2022Isnara Pereira IvoAinda não há avaliações
- Ficha Trimestral 3Documento3 páginasFicha Trimestral 3Isnara Pereira IvoAinda não há avaliações
- Informes ReuniãoDocumento2 páginasInformes ReuniãoIsnara Pereira IvoAinda não há avaliações
- Tese Isabel Familai EscravaDocumento305 páginasTese Isabel Familai EscravaIsnara Pereira IvoAinda não há avaliações
- SLENES Robert Na Senzala Uma Flor EsperaDocumento2 páginasSLENES Robert Na Senzala Uma Flor EsperaIsnara Pereira IvoAinda não há avaliações
- Na Senzala Uma Flor Esperancas Na Formacao Da Fami PDFDocumento5 páginasNa Senzala Uma Flor Esperancas Na Formacao Da Fami PDFFabiana MeloAinda não há avaliações
- Livrs de Cor Na MartinicaDocumento26 páginasLivrs de Cor Na MartinicaIsnara Pereira IvoAinda não há avaliações
- Tese Rodrigo C ResendeDocumento397 páginasTese Rodrigo C ResendeIsnara Pereira IvoAinda não há avaliações
- Dicionário de Negreiros em Moçambique - José Capela PDFDocumento254 páginasDicionário de Negreiros em Moçambique - José Capela PDFalgoz36Ainda não há avaliações
- Livrs de Cor Na MartinicaDocumento26 páginasLivrs de Cor Na MartinicaIsnara Pereira IvoAinda não há avaliações
- 242 Questões de EnfemagemDocumento70 páginas242 Questões de EnfemagemjanaraAinda não há avaliações
- Aplicação de Técnicas de Aprendizagem de Máquina para Diagnóstico de Depressão, Ansiedade e EstresseDocumento4 páginasAplicação de Técnicas de Aprendizagem de Máquina para Diagnóstico de Depressão, Ansiedade e EstresseJuliana Cristina de AndradeAinda não há avaliações
- Nutricosmeticos e MelasmaDocumento12 páginasNutricosmeticos e MelasmaAline Brito Ferreira de CastroAinda não há avaliações
- Planilha de Avaliação Da Composição CorporalDocumento1 páginaPlanilha de Avaliação Da Composição CorporalluanagomeslopesAinda não há avaliações
- Monografia CompletaDocumento36 páginasMonografia CompletaCarolina DavidAinda não há avaliações
- Cintura Pélvica - Incidências EspeciaisDocumento24 páginasCintura Pélvica - Incidências EspeciaisNorton FontellaAinda não há avaliações
- Elementos Da PedagogiaDocumento10 páginasElementos Da PedagogiaTeodósio Cipriano SilvérioAinda não há avaliações
- O Uso de Substâncias Psicoativas e A FamíliaDocumento9 páginasO Uso de Substâncias Psicoativas e A FamíliaRaquel CardosoAinda não há avaliações
- Depressão - Clínica, Crítica e Ética - Orlando CoserDocumento168 páginasDepressão - Clínica, Crítica e Ética - Orlando CoserPatricia SanthosAinda não há avaliações
- Projeto Abastecimento de Agua Cidade Jardim-GoDocumento9 páginasProjeto Abastecimento de Agua Cidade Jardim-GoAmanda OLiveira100% (1)
- Uma Compreensão Sobre o PsicodramaDocumento3 páginasUma Compreensão Sobre o PsicodramajpcidturAinda não há avaliações
- 2243 - Perna Bipartida em V 500 550Documento1 página2243 - Perna Bipartida em V 500 550Carlos Luciano Cardoso De AraujoAinda não há avaliações
- AnemiaDocumento15 páginasAnemiamaysapg100% (2)
- SEI - MS - 0015478345 - OfícioDocumento3 páginasSEI - MS - 0015478345 - OfícioLeonardo MeirelesAinda não há avaliações
- Resumo Coberturas, Produtos Feridas BasesDocumento20 páginasResumo Coberturas, Produtos Feridas BasesCecília OliveiraAinda não há avaliações
- Apostila Teoria Semiologia PDFDocumento34 páginasApostila Teoria Semiologia PDFAnonymous rqVEVIuEY100% (3)
- Teste de ContatoDocumento10 páginasTeste de Contatodaniel oliveiraAinda não há avaliações
- MANUAL DE SOBREVIVÊNCIA PSÍQUICA EM TEMPOS DE CRISE - A Ciência Ajuda Você A Realizar Seus Planos - REVISTA MENTE CÉREBRO, ESPECIAL N. 51Documento7 páginasMANUAL DE SOBREVIVÊNCIA PSÍQUICA EM TEMPOS DE CRISE - A Ciência Ajuda Você A Realizar Seus Planos - REVISTA MENTE CÉREBRO, ESPECIAL N. 51Karla Juliana dos Santos CavalcantiAinda não há avaliações
- Calculadora Do Tamanho Do Bebê Fetalmed - Medicina Fetal em CuritibaDocumento1 páginaCalculadora Do Tamanho Do Bebê Fetalmed - Medicina Fetal em CuritibaLarissa CastroAinda não há avaliações
- Termo de Adesão Ao Plano de Saúde Hapvida AtualizadoDocumento1 páginaTermo de Adesão Ao Plano de Saúde Hapvida AtualizadoAristoteles WagnerAinda não há avaliações
- Grandes e Hipercoradas Nas Anemias MegaloblásticasDocumento2 páginasGrandes e Hipercoradas Nas Anemias MegaloblásticasJohn mc MaddenAinda não há avaliações
- Saber Popular e Saber CientíficoDocumento3 páginasSaber Popular e Saber CientíficoFábio Nascimento100% (1)
- Fibromialgia Sem Misterio PDFDocumento11 páginasFibromialgia Sem Misterio PDFpriscilaAinda não há avaliações
- CFB 6ano 2bimestreDocumento2 páginasCFB 6ano 2bimestreJosi AlvesAinda não há avaliações
- Desenvolvimento de Modelo de Acompanhamento Farmacoterapêutico A Pacientes Com Câncer de Mama Metastático em Tratamento Com CapecitabinaDocumento23 páginasDesenvolvimento de Modelo de Acompanhamento Farmacoterapêutico A Pacientes Com Câncer de Mama Metastático em Tratamento Com CapecitabinaIone Cristina MenesesAinda não há avaliações
- Avaliação Da Saúde Ocular Un 1Documento105 páginasAvaliação Da Saúde Ocular Un 1JOSIANEAinda não há avaliações
- O Uso de Técnicas de Relaxamento para Sintomas Ansiosos PDFDocumento59 páginasO Uso de Técnicas de Relaxamento para Sintomas Ansiosos PDFAmanda Bosnich Dos Santos100% (1)
- Livro - Estimulação Precoce 1Documento24 páginasLivro - Estimulação Precoce 1Alissafel0% (1)
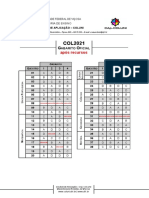
- COL2021 Gabarito - Oficial RECURSOSDocumento1 páginaCOL2021 Gabarito - Oficial RECURSOSGiulia cruzeiraoAinda não há avaliações
- Manual para Os Serviços de Saúde Dos Servidores Civis FederaisDocumento47 páginasManual para Os Serviços de Saúde Dos Servidores Civis FederaisAirton MarinhoAinda não há avaliações