Você também pode gostar
- Demências e Parkinsonismo 2Documento14 páginasDemências e Parkinsonismo 2Suellen Mayumy Ichitani100% (1)
- Demência progressiva em homem de 43 anosDocumento4 páginasDemência progressiva em homem de 43 anosPedro Foliatti de AzevedoAinda não há avaliações
- Caso 13Documento7 páginasCaso 13Mel martinsAinda não há avaliações
- 6 FD 533Documento45 páginas6 FD 533Tuane de OliveiraAinda não há avaliações
- Afasia Global Sem Hemiparesia AVC Ou Transtorno ConversivoDocumento6 páginasAfasia Global Sem Hemiparesia AVC Ou Transtorno ConversivoMiguel SorianiAinda não há avaliações
- Doença de Alzheimer. Como Identificar, Prevenir e TratarDocumento8 páginasDoença de Alzheimer. Como Identificar, Prevenir e TratarJuniorAinda não há avaliações
- Doença de HuntingtonDocumento4 páginasDoença de HuntingtonchiclebluejmAinda não há avaliações
- Doença de Alzheimer Artigo de 2021Documento26 páginasDoença de Alzheimer Artigo de 2021Lidiane AbreuAinda não há avaliações
- Doença de Alzheimer: aspectos clínicos e diagnósticosDocumento12 páginasDoença de Alzheimer: aspectos clínicos e diagnósticosAlessandro Miland Rodrigues Do ValeAinda não há avaliações
- Biologia molecular da doença de AlzheimerDocumento7 páginasBiologia molecular da doença de AlzheimerGabriel Nunes da SilvaAinda não há avaliações
- Aula 9 - Doença de AlzheimerDocumento51 páginasAula 9 - Doença de AlzheimerCamila RoldanAinda não há avaliações
- Doença de Hungtinton - Uma Revisão Dos Aspectos FisiopatológicosDocumento11 páginasDoença de Hungtinton - Uma Revisão Dos Aspectos FisiopatológicosMariana CoelhoAinda não há avaliações
- Stevensε DekabanDocumento17 páginasStevensε DekabanLaura Giovanna WebrathAinda não há avaliações
- Atualização sobre a Síndrome de RettDocumento4 páginasAtualização sobre a Síndrome de RettadilsonkingAinda não há avaliações
- MitocondriopatiasDocumento58 páginasMitocondriopatiasjoseAinda não há avaliações
- Sindrome CADASILDocumento33 páginasSindrome CADASILEduardo NolascoAinda não há avaliações
- Avaliação Neuropsicológica Na Doença de Alzheimer E No Comprometimento Cognitivo LeveDocumento11 páginasAvaliação Neuropsicológica Na Doença de Alzheimer E No Comprometimento Cognitivo LeveThaíssa Ágatha BaraunaAinda não há avaliações
- X BJ7 MMV BEWHp 17 ZE6 y ZCWJYDih Z0Documento2 páginasX BJ7 MMV BEWHp 17 ZE6 y ZCWJYDih Z0Re FerreiraAinda não há avaliações
- Neurologia Pediátrica COREME UNIFESP 2014Documento8 páginasNeurologia Pediátrica COREME UNIFESP 2014Beatriz DiasAinda não há avaliações
- Relato de caso de doença de Creutzfeldt-JakobDocumento4 páginasRelato de caso de doença de Creutzfeldt-JakobMariano David Díaz GambiniAinda não há avaliações
- Relato de caso de infarto da artéria de PercheronDocumento4 páginasRelato de caso de infarto da artéria de PercheronFIAMAAinda não há avaliações
- Uso de Canabinoides Como Adjuvante No Tratamento Da Doença de AlzheimerDocumento8 páginasUso de Canabinoides Como Adjuvante No Tratamento Da Doença de Alzheimerrrrcavalcante.artAinda não há avaliações
- Aspectos neurológicos na síndrome da criança espancadaDocumento6 páginasAspectos neurológicos na síndrome da criança espancadaBruce MarlonAinda não há avaliações
- Demência ScieloDocumento4 páginasDemência ScieloClayton Carstens Jr.Ainda não há avaliações
- Doenças NeurodegenerativasDocumento8 páginasDoenças NeurodegenerativasengsetbrAinda não há avaliações
- Zamora Ambar Caso Clinico ComaDocumento15 páginasZamora Ambar Caso Clinico ComaRoxanaAinda não há avaliações
- NEUROLOGIADocumento8 páginasNEUROLOGIAjuliana oliveiraAinda não há avaliações
- Mecanismos Fisiopatógicos Do DeliriumDocumento9 páginasMecanismos Fisiopatógicos Do DeliriumxerfanAinda não há avaliações
- Doenças do Sistema Nervoso: AVC, Alzheimer e maisDocumento16 páginasDoenças do Sistema Nervoso: AVC, Alzheimer e maismadalena martinsAinda não há avaliações
- Caso ClinicoDocumento9 páginasCaso ClinicoFelipe CostaAinda não há avaliações
- Como Diagnosticar As Quatro Causas Mais Freqüentes de DemênciaDocumento4 páginasComo Diagnosticar As Quatro Causas Mais Freqüentes de DemênciaJosiane AlmeidaAinda não há avaliações
- Avaliação Neuro Adulto IIDocumento89 páginasAvaliação Neuro Adulto IIpsicologaAinda não há avaliações
- O Exercício e A Doenças de AlzheimerDocumento10 páginasO Exercício e A Doenças de AlzheimerJuniorAinda não há avaliações
- Fisiopatologia Da Doença de Alzheimer e Os Quatro Genes Associados A DoençaDocumento22 páginasFisiopatologia Da Doença de Alzheimer e Os Quatro Genes Associados A DoençaVITORIA PIRESAinda não há avaliações
- 189716-Texto Do Artigo-565274-1-10-20220706Documento7 páginas189716-Texto Do Artigo-565274-1-10-20220706João Manoel Sousa SoaresAinda não há avaliações
- Demências e parkinsonismo: diagnóstico e principais causasDocumento26 páginasDemências e parkinsonismo: diagnóstico e principais causasElizeu Eschenmoser DominguezAinda não há avaliações
- Sindrome Top de La BasilarDocumento4 páginasSindrome Top de La BasilarCarlos Ruiz HidalgoAinda não há avaliações
- Fichamento sobre traumatismo craniano, AVE, epilepsia, autismo, Parkinson e AlzheimerDocumento4 páginasFichamento sobre traumatismo craniano, AVE, epilepsia, autismo, Parkinson e AlzheimerLuis AlexandreAinda não há avaliações
- Aula Alzheimer 2020Documento25 páginasAula Alzheimer 2020jessica moreiraAinda não há avaliações
- Temas para Seminários 2021Documento5 páginasTemas para Seminários 2021Sthefanny AlvesAinda não há avaliações
- 19194-Texto Do Artigo-52671-1-2-20210705Documento10 páginas19194-Texto Do Artigo-52671-1-2-20210705Nathalia soares leandroAinda não há avaliações
- Miopatias Vs Miastenia A Congresso Abmfr 2008Documento24 páginasMiopatias Vs Miastenia A Congresso Abmfr 2008Regina ReginaAinda não há avaliações
- Alzheimer - FinalDocumento66 páginasAlzheimer - FinalGilberto Augusto100% (1)
- Ataxias Agudas e SubagudasDocumento38 páginasAtaxias Agudas e Subagudasguilherme.chaparimAinda não há avaliações
- Demência: Síndrome de declínio cognitivoDocumento4 páginasDemência: Síndrome de declínio cognitivoMarina100% (1)
- Material de Estudo Processo Seletivo LAMEI-UFJF - 231204 - 221122Documento60 páginasMaterial de Estudo Processo Seletivo LAMEI-UFJF - 231204 - 221122Nathany ÁvilaAinda não há avaliações
- Artigo 119422 3 10 20220713Documento8 páginasArtigo 119422 3 10 20220713gabrielmorais1999Ainda não há avaliações
- Síndrome de MenkesDocumento12 páginasSíndrome de MenkesGlam UpAinda não há avaliações
- Resumo ProvaDocumento10 páginasResumo ProvaMarcela MachadoAinda não há avaliações
- VIVA COM EPILEPSIA Epilepsia No IdosoDocumento8 páginasVIVA COM EPILEPSIA Epilepsia No IdosoIvan CarvalhoAinda não há avaliações
- 1693003410178+1692961811862+estudo Dirigido 072023 - AtualizadoDocumento12 páginas1693003410178+1692961811862+estudo Dirigido 072023 - AtualizadoSofia Barbosa LimaAinda não há avaliações
- A Linha Ténue Entre A Demência e Depressão No IdosoDocumento7 páginasA Linha Ténue Entre A Demência e Depressão No IdosoMiguel PlenoAinda não há avaliações
- Vf33-Texto Do Artigo-193-216-10-20200429Documento9 páginasVf33-Texto Do Artigo-193-216-10-20200429Leila HashimotoAinda não há avaliações
- ARP 2005-1-73 Algoneurodistrofia Jan-Mar 05Documento8 páginasARP 2005-1-73 Algoneurodistrofia Jan-Mar 05Inês GuedesAinda não há avaliações
- Patologia AV1Documento19 páginasPatologia AV1Artur MenezesAinda não há avaliações
- Revisão literária da doença de Alzheimer: o impacto no âmbito familiarNo EverandRevisão literária da doença de Alzheimer: o impacto no âmbito familiarAinda não há avaliações
- Apostila de NeurologiaDocumento68 páginasApostila de NeurologiaLuciana E Túlio100% (2)
- Síndrome da cabeça caída em pacientes com doença do neurônio motorDocumento4 páginasSíndrome da cabeça caída em pacientes com doença do neurônio motorMarceloAinda não há avaliações
- os DISTÚRBIOS NEUROLÓGICOSNo Everandos DISTÚRBIOS NEUROLÓGICOSAinda não há avaliações
- Doenças de Notificação Compulsória 2021Documento4 páginasDoenças de Notificação Compulsória 2021Beatriz Gomes RibeiroAinda não há avaliações
- Teixeira, Carmen. Cap. 6 Planejamento em SaudeDocumento43 páginasTeixeira, Carmen. Cap. 6 Planejamento em SaudeANÔNIMOAinda não há avaliações
- ENTREGUE 1302atividade Presencial 16-Acao em Vigilancia e SaudeDocumento2 páginasENTREGUE 1302atividade Presencial 16-Acao em Vigilancia e SaudeDeivson Ferreira100% (2)
- Trabalho de Fundamentos de Estatística e EpidemiologiaDocumento7 páginasTrabalho de Fundamentos de Estatística e EpidemiologiaTommyWilliamesAinda não há avaliações
- História Natural Da Covid-19 E Suas Relações Terapêuticas: Abel Silva de MenesesDocumento10 páginasHistória Natural Da Covid-19 E Suas Relações Terapêuticas: Abel Silva de MenesesAna Carla Piasecki da CostaAinda não há avaliações
- Exemplo Ficha Pesquisa BibliograficaDocumento4 páginasExemplo Ficha Pesquisa BibliograficadoglasnegriAinda não há avaliações
- Transc. PSFDocumento240 páginasTransc. PSFSuelen LimaAinda não há avaliações
- LemonDocumento1 páginaLemonJaquelyne HenkeesAinda não há avaliações
- Anamnese - RoteiroDocumento2 páginasAnamnese - RoteiroRoberta GondimAinda não há avaliações
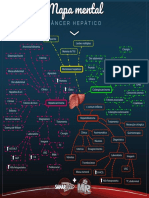
- MapamentalCncerHeptico1546466666106 1554402321672Documento1 páginaMapamentalCncerHeptico1546466666106 1554402321672Alejandro Josue Zurita ChucaAinda não há avaliações
- Nefropatia Por HIVDocumento38 páginasNefropatia Por HIVhugo benedito hugoAinda não há avaliações
- Análise multidimensional das causas múltiplas de morte por doenças crônico-degenerativasDocumento9 páginasAnálise multidimensional das causas múltiplas de morte por doenças crônico-degenerativasMaria ArgoloAinda não há avaliações
- PRR - Doenças do TrabalhoDocumento3 páginasPRR - Doenças do TrabalhoTatiana Rodegheri100% (4)
- Artrite Psoriásica: Características, Diagnóstico e TratamentoDocumento31 páginasArtrite Psoriásica: Características, Diagnóstico e TratamentoYasmine FortesAinda não há avaliações
- Dor aguda Chikungunya fluxograma tratamentoDocumento5 páginasDor aguda Chikungunya fluxograma tratamentoJosenildo Firmino FirminoAinda não há avaliações
- Promovendo a saúde através da atividade físicaDocumento28 páginasPromovendo a saúde através da atividade físicaMarcos MoraesAinda não há avaliações
- HIV-Vírus ImunodeficiênciaDocumento15 páginasHIV-Vírus ImunodeficiênciaLuciana Pereira da SilvaAinda não há avaliações
- Levantamento epidemiológico de CPO-D em crianças da escola CAIC-ALDocumento15 páginasLevantamento epidemiológico de CPO-D em crianças da escola CAIC-ALKeyla MoraisAinda não há avaliações
- Boas Práticas de Farmacovigilância - AméricasDocumento85 páginasBoas Práticas de Farmacovigilância - Américas235211028Ainda não há avaliações
- DPOC - Doença Pulmonar Obstrutiva CrônicaDocumento27 páginasDPOC - Doença Pulmonar Obstrutiva Crônicawinni RamosAinda não há avaliações
- Edema Agudo de PulmãoDocumento9 páginasEdema Agudo de PulmãoAlexandre Oliveira100% (1)
- Doenças ExantemáticasDocumento24 páginasDoenças ExantemáticasAdejaime AssunçaoAinda não há avaliações
- Folder MaláriaDocumento1 páginaFolder MaláriaVIGILANCIA ATM ATMAinda não há avaliações
- Slide MicrobiologiaDocumento23 páginasSlide MicrobiologiaSara BeatrizAinda não há avaliações
- Doenças de Notificação CompulsoriaDocumento3 páginasDoenças de Notificação CompulsoriacelenandaAinda não há avaliações
- Importância Das Vacinas e Dos SorosDocumento4 páginasImportância Das Vacinas e Dos SorosAdriano CardosoAinda não há avaliações
- Medidas de Tendencia Central - Aula5Documento20 páginasMedidas de Tendencia Central - Aula5Edilson Valente JotteAinda não há avaliações
- Estudo Dirigido P1Documento3 páginasEstudo Dirigido P1Flávia SantosAinda não há avaliações
- Diário República 229 2013Documento3 páginasDiário República 229 2013Catarina MoreiraAinda não há avaliações
- Manual de Clínica Médica - InfectologiaDocumento71 páginasManual de Clínica Médica - InfectologiaNAARA SILVA GUERRAAinda não há avaliações