Você também pode gostar
- Fraturas Do Fêmur ProximalDocumento52 páginasFraturas Do Fêmur ProximalEduardo PaesAinda não há avaliações
- Tratamento de Fraturas do AstrágaloDocumento44 páginasTratamento de Fraturas do AstrágaloHamilton SaideAinda não há avaliações
- Prova 5Documento24 páginasProva 5AsdfAinda não há avaliações
- Aula .Fratura Trocanterica HuDocumento42 páginasAula .Fratura Trocanterica HuIgor Gerdi OppeAinda não há avaliações
- Imagiologia e HemodinâmicaDocumento25 páginasImagiologia e HemodinâmicaCinthya Carlene Terapias NaturaisAinda não há avaliações
- Fraturas Do Planalto TibialDocumento26 páginasFraturas Do Planalto TibialAllanOno100% (3)
- 1 Skills 2013Documento168 páginas1 Skills 2013Clínica de Medicina Dentária Drª Fernanda ToméAinda não há avaliações
- Pelve InfantilDocumento28 páginasPelve InfantilFabio YamaguchiAinda não há avaliações
- Prova 1 Rusumo TeotDocumento37 páginasProva 1 Rusumo Teotyamila100% (1)
- Fraturas e LuxaçõesDocumento22 páginasFraturas e LuxaçõesIsabela OliveiraAinda não há avaliações
- Prova 4Documento29 páginasProva 4AsdfAinda não há avaliações
- Prova 1Documento37 páginasProva 1AsdfAinda não há avaliações
- Fraturas Da Extremidade Proximal Da Tíbia e Da FíbulaDocumento56 páginasFraturas Da Extremidade Proximal Da Tíbia e Da FíbulaDennis SansanoviczAinda não há avaliações
- Lesões ortopédicas e traumatológicas na prova 1Documento37 páginasLesões ortopédicas e traumatológicas na prova 1Lana Lacerda de LimaAinda não há avaliações
- Fraturas MMSSDocumento46 páginasFraturas MMSSapi-3705422100% (5)
- Aula Pré-OperatorioDocumento66 páginasAula Pré-OperatorioPriscilla Manhães GomesAinda não há avaliações
- Quadril 10 Mil QuestõesDocumento79 páginasQuadril 10 Mil QuestõeseddieAinda não há avaliações
- Aula SD Compart. e ExpostaDocumento43 páginasAula SD Compart. e ExpostaJorge AiresAinda não há avaliações
- Traumavascular 120904143107 Phpapp02Documento91 páginasTraumavascular 120904143107 Phpapp02Matt LazardAinda não há avaliações
- Doenca de KienbockDocumento11 páginasDoenca de KienbockrobertowanderlanAinda não há avaliações
- Lesões ortopédicas e deformidadesDocumento30 páginasLesões ortopédicas e deformidadesLana Lacerda de LimaAinda não há avaliações
- Cirurgia de Ressutura Do EsternoDocumento11 páginasCirurgia de Ressutura Do EsternoSabrina VieiraAinda não há avaliações
- Trauma Ped 23-2Documento99 páginasTrauma Ped 23-2lucasdelphim234Ainda não há avaliações
- Anestesias loco-regionais: agentes anestésicos e efeitos fisiológicosDocumento28 páginasAnestesias loco-regionais: agentes anestésicos e efeitos fisiológicosMargarida ReisAinda não há avaliações
- TX Renal Santa MarcelinaDocumento51 páginasTX Renal Santa MarcelinaSeleno GlauberAinda não há avaliações
- TireoidectomiaDocumento30 páginasTireoidectomiaAmanda GarciaAinda não há avaliações
- Protocol oDocumento196 páginasProtocol oRafael RezendeAinda não há avaliações
- Apresentação 1Documento13 páginasApresentação 1q5pbf5mjmbAinda não há avaliações
- AmputaçãoDocumento131 páginasAmputaçãoThamara Benjamim100% (1)
- Doença de KienböckDocumento5 páginasDoença de KienböckThemisPinheiroAinda não há avaliações
- Câncer de pâncreas: tratamento cirúrgico e complicações da WhippleDocumento50 páginasCâncer de pâncreas: tratamento cirúrgico e complicações da WhippleRenan MirandaAinda não há avaliações
- Aula Traumatoortopedia - QuadrilDocumento64 páginasAula Traumatoortopedia - QuadrilLeandro LimaAinda não há avaliações
- Tratamento Da Síndrome Do Ligamento Arqueado Mediano - Resultado Da Abordagem LaporascópicaDocumento4 páginasTratamento Da Síndrome Do Ligamento Arqueado Mediano - Resultado Da Abordagem LaporascópicaLiah LopesAinda não há avaliações
- Manual de Cirurgias Eletivas da Santa Casa de Misericórdia de SobralNo EverandManual de Cirurgias Eletivas da Santa Casa de Misericórdia de SobralAinda não há avaliações
- Fracturas Da Extremidade Distal Do AntebraçoDocumento38 páginasFracturas Da Extremidade Distal Do AntebraçoEunice_C100% (1)
- FRATURAS SUBTROCANTERICAS: EPIDEMIOLOGIA, CLASSIFICAÇÃO E TRATAMENTODocumento28 páginasFRATURAS SUBTROCANTERICAS: EPIDEMIOLOGIA, CLASSIFICAÇÃO E TRATAMENTOGivanildo SoaresAinda não há avaliações
- Implante Percutâneo de Endoprótese Valvar Aórtica - Fundamentos e Seleção Dos CandidatosDocumento48 páginasImplante Percutâneo de Endoprótese Valvar Aórtica - Fundamentos e Seleção Dos CandidatosJorge BragaAinda não há avaliações
- Anatomia Radiológica Punho e MãoDocumento39 páginasAnatomia Radiológica Punho e Mãoferpae100% (1)
- Fratura de calcâneo: classificação e tratamentoDocumento76 páginasFratura de calcâneo: classificação e tratamentoRenan BarataAinda não há avaliações
- Slides - Aneurisma de Aorta AbdominalDocumento24 páginasSlides - Aneurisma de Aorta AbdominalAillyn BianchiAinda não há avaliações
- 1 SKILLS 2013 Casos ClinicosDocumento16 páginas1 SKILLS 2013 Casos ClinicosClínica de Medicina Dentária Drª Fernanda ToméAinda não há avaliações
- Aula Fadiga CorrigidaDocumento193 páginasAula Fadiga Corrigidafrancisco.l.castro147Ainda não há avaliações
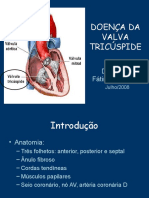
- Doença da valva tricúspide: etiologias, apresentação clínica, manejo e cirurgiaDocumento25 páginasDoença da valva tricúspide: etiologias, apresentação clínica, manejo e cirurgiaMaria Rafaela AndradeAinda não há avaliações
- TIREOIDECTOMIADocumento30 páginasTIREOIDECTOMIACaio Amaral0% (1)
- Curso de Cirurgia Geral sobre Diverticulite AgudaDocumento43 páginasCurso de Cirurgia Geral sobre Diverticulite AgudaLigia CanovaAinda não há avaliações
- Tumores Do Esôfago: Prof Cecilia Alcantara Braga GarciaDocumento43 páginasTumores Do Esôfago: Prof Cecilia Alcantara Braga GarciaThiago CunhaAinda não há avaliações
- Fraturas de Tíbia e Fíbula ProximaisDocumento42 páginasFraturas de Tíbia e Fíbula ProximaisMárcio SilveiraAinda não há avaliações
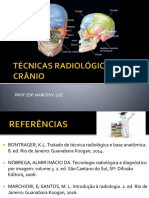
- Radiologia crânio-encefálicaDocumento39 páginasRadiologia crânio-encefálicaMarcosviniciusluz100% (1)
- Psa EscafoideDocumento62 páginasPsa EscafoideLorraine DuarteAinda não há avaliações
- Fratura de Femur Resumo Ortopedia 2019Documento4 páginasFratura de Femur Resumo Ortopedia 2019fabiictAinda não há avaliações
- (P) 2023 - 0008 - RC - Mody Et Al - inDocumento6 páginas(P) 2023 - 0008 - RC - Mody Et Al - inGirish RAinda não há avaliações
- Cistectomia RadicalDocumento28 páginasCistectomia RadicalcleybismarAinda não há avaliações
- Fratura Do Umero ProximalDocumento77 páginasFratura Do Umero ProximalRafael Teixeira FernandesAinda não há avaliações
- Bases da Laparoscopia: Procedimentos Cirúrgicos Minimamente InvasivosDocumento130 páginasBases da Laparoscopia: Procedimentos Cirúrgicos Minimamente InvasivosCleiton Rodrigues100% (2)
- Fratura OmbroDocumento39 páginasFratura OmbroTalita SáAinda não há avaliações
- Artroplastia de JoelhoDocumento53 páginasArtroplastia de JoelhoMárcio SilveiraAinda não há avaliações
- Fratura Umero ProximalDocumento59 páginasFratura Umero ProximalMárcio SilveiraAinda não há avaliações
- Amputa º ÁesDocumento80 páginasAmputa º ÁesCesar LimaAinda não há avaliações
- Lesao de Antebraço Punho e Mao NOVO 2Documento69 páginasLesao de Antebraço Punho e Mao NOVO 2elianeAinda não há avaliações
- Apostila de MatemáticaDocumento10 páginasApostila de MatemáticaJosineide AndradeAinda não há avaliações
- Plano Diretor AtualDocumento54 páginasPlano Diretor AtualWillian NovaesAinda não há avaliações
- A lição do abacaxiDocumento3 páginasA lição do abacaxiJunior John Erich Da SilvaAinda não há avaliações
- Beneficios Da Acupuntura Na Terceira IdadeDocumento15 páginasBeneficios Da Acupuntura Na Terceira IdadeNilton BragaAinda não há avaliações
- Avaliação de Ciências 5º Ano 1º BDocumento4 páginasAvaliação de Ciências 5º Ano 1º Bvaleria cristina de souzaAinda não há avaliações
- Apostila 14 CAD Conceitos BasicosDocumento4 páginasApostila 14 CAD Conceitos BasicosJardel JuniorAinda não há avaliações
- A Psicologia Da Educação e Seus Elementos Essenciais - AtivDocumento7 páginasA Psicologia Da Educação e Seus Elementos Essenciais - AtivPatrice HellenAinda não há avaliações
- O Conceito de Região em Três Registros. Exemplificando Com o Nordeste BrasileiroDocumento11 páginasO Conceito de Região em Três Registros. Exemplificando Com o Nordeste Brasileirocelio soaresAinda não há avaliações
- Problemas Ambientais 2020Documento8 páginasProblemas Ambientais 2020Adão Marcos GracianoAinda não há avaliações
- PEDAGOGIA INTEGRADA MatériaDocumento18 páginasPEDAGOGIA INTEGRADA MatériaMilenaAinda não há avaliações
- Excel Avançado: Funções e Ferramentas PoderosasDocumento41 páginasExcel Avançado: Funções e Ferramentas PoderosasJaqueline SilvaAinda não há avaliações
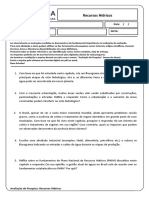
- Recursos HidricosDocumento2 páginasRecursos HidricosLucideia Alonso0% (1)
- Candido 73Documento40 páginasCandido 73Alisson OliveiraAinda não há avaliações
- RUÍDO NO AMBIENTE DE TRABALHODocumento6 páginasRUÍDO NO AMBIENTE DE TRABALHOrodri23Ainda não há avaliações
- Biblioteca Escolar (39950)Documento5 páginasBiblioteca Escolar (39950)Nilson CortesAinda não há avaliações
- Tecnologias de Informação e ComunicaçãoDocumento12 páginasTecnologias de Informação e ComunicaçãoSergioMatsoloAinda não há avaliações
- Gestão de estoques: funções, custos e controleDocumento121 páginasGestão de estoques: funções, custos e controlePedro HenriqueAinda não há avaliações
- História Da Moda Da Idade Média À Contemporaneidade Do Acervo Bibliográfico Do Senac - Campus Santo AmaroDocumento11 páginasHistória Da Moda Da Idade Média À Contemporaneidade Do Acervo Bibliográfico Do Senac - Campus Santo AmaroCidinha PinheiroAinda não há avaliações
- Controle Display Cristal LíquidoDocumento14 páginasControle Display Cristal LíquidoEmerson ReisAinda não há avaliações
- Actas-ENEC-2007-Contributos para A Qualidade Educativa No Ensino Das Ciências Do Pré-Escolar Ao SuperiorDocumento684 páginasActas-ENEC-2007-Contributos para A Qualidade Educativa No Ensino Das Ciências Do Pré-Escolar Ao SuperiorLeonel MorgadoAinda não há avaliações
- 2.2.1-Pot1 Sist3F AbilioDocumento48 páginas2.2.1-Pot1 Sist3F AbilioDanilo Do ValleAinda não há avaliações
- Gincana Estudantil sobre Folclore BrasileiroDocumento11 páginasGincana Estudantil sobre Folclore Brasileirovaldirene rodriguesAinda não há avaliações
- Textos de inspiração para o coraçãoDocumento23 páginasTextos de inspiração para o coraçãoJoysse Campanha PsicólogaAinda não há avaliações
- Tradução G-CodeDocumento7 páginasTradução G-CodeJean Neves dos Santos SerraAinda não há avaliações
- Magnetismo - Estudo da atração e repulsão de objetos magnéticosDocumento5 páginasMagnetismo - Estudo da atração e repulsão de objetos magnéticosMoisés Nunes MoreiraAinda não há avaliações
- 2S036A0000S00Documento162 páginas2S036A0000S00Miguel DiasAinda não há avaliações
- Relatório Gerador de Van Der GraffDocumento7 páginasRelatório Gerador de Van Der GraffBrenda CamposAinda não há avaliações
- Comprovante ViniciusDocumento1 páginaComprovante Viniciusrayla23560% (1)
- A Escrita Da História - Peter BurkeDocumento2 páginasA Escrita Da História - Peter BurkeNatália CorrêaAinda não há avaliações
- Rdo Rev.12 07 18Documento2 páginasRdo Rev.12 07 18Cassio CostaAinda não há avaliações