Você também pode gostar
- Isso Não Começou Com Você (Traduz.) - Mark WolynnDocumento219 páginasIsso Não Começou Com Você (Traduz.) - Mark WolynnFabiana85% (26)
- Relatório de Estágio em Alimentação ColetivaDocumento97 páginasRelatório de Estágio em Alimentação ColetivaValéria Tarelho100% (6)
- Appcc Doce LeiteDocumento24 páginasAppcc Doce LeiteLaís Maria FerreiraAinda não há avaliações
- Roteiro para Vender Através Do StoriesDocumento31 páginasRoteiro para Vender Através Do Storiesluamsmarins100% (1)
- Folder Uso Do EPIDocumento2 páginasFolder Uso Do EPIvsouzajunior100% (2)
- Caso Pratico Guia Anvisa - CRF GO PDFDocumento54 páginasCaso Pratico Guia Anvisa - CRF GO PDFWilliam Salgado100% (1)
- PPRA - Comercio de AlimentosDocumento10 páginasPPRA - Comercio de AlimentosFabio FerreiraAinda não há avaliações
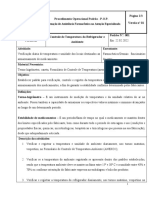
- Pop TemperaturaDocumento8 páginasPop TemperaturaAna Cláudia SobralAinda não há avaliações
- POP 08 - Recolhimento de Produtos PDFDocumento9 páginasPOP 08 - Recolhimento de Produtos PDFMaya Sato100% (3)
- Relatório de Estágio Obrigatório ElinaDocumento24 páginasRelatório de Estágio Obrigatório ElinaCesar Botelho100% (1)
- Apometria Jose Lacerda de Azevedo Energia e EspritoDocumento117 páginasApometria Jose Lacerda de Azevedo Energia e Espritogisele.aa16507100% (4)
- O Fim Da GastriteDocumento120 páginasO Fim Da Gastritevictor oliveiraAinda não há avaliações
- Menino de AsasDocumento15 páginasMenino de AsasUnidade Escolar Rosa MísticaAinda não há avaliações
- São João Batista Maria Vianney - Biografia, Obras, Espiritualidade - Edemir Lopes de Souza PDFDocumento15 páginasSão João Batista Maria Vianney - Biografia, Obras, Espiritualidade - Edemir Lopes de Souza PDFViam prudentiae100% (2)
- 023-Protocolo SepseDocumento3 páginas023-Protocolo SepseMatheus VerasAinda não há avaliações
- Passo A Passo Da Coleta de Alimentos Com Suspeita de DtaDocumento5 páginasPasso A Passo Da Coleta de Alimentos Com Suspeita de Dtakatia andradeAinda não há avaliações
- POP Sala de Vacina Ubs AcaciasDocumento24 páginasPOP Sala de Vacina Ubs AcaciasUSF ACACIASAinda não há avaliações
- Documentos e RegistrosDocumento9 páginasDocumentos e RegistrosCláudio HieltsinAinda não há avaliações
- 2022 Planilha POP 1B - Controle de RecebimentoDocumento2 páginas2022 Planilha POP 1B - Controle de RecebimentoBrenda FerreiraAinda não há avaliações
- Manual ColetaDocumento19 páginasManual Coletaapi-3704990100% (1)
- 5.2 Código Boas PráticasDocumento17 páginas5.2 Código Boas PráticasLiliana AlmeidaAinda não há avaliações
- Condições de Temperatura Produtos Equipe de EntregaDocumento2 páginasCondições de Temperatura Produtos Equipe de EntregaAndressa MariaAinda não há avaliações
- MA04008C - Avaliação Do Poder AntissépticoDocumento4 páginasMA04008C - Avaliação Do Poder AntissépticoEduardo AlencarAinda não há avaliações
- Coleta e Amostras de Alimentos em Unidade de AlimentaçãoDocumento18 páginasColeta e Amostras de Alimentos em Unidade de Alimentaçãosuanam tavaresAinda não há avaliações
- Qualificação de TransporteDocumento55 páginasQualificação de TransportePRISCILA FERNANDA SOUZAAinda não há avaliações
- Orientações COVID 19Documento15 páginasOrientações COVID 19PamelaAinda não há avaliações
- Estudo de Caso - Aplicação Do PDCA em Um LaticínioDocumento2 páginasEstudo de Caso - Aplicação Do PDCA em Um Laticíniojaqueline baldezAinda não há avaliações
- Sala de Vacina eDocumento91 páginasSala de Vacina eCecília SantosAinda não há avaliações
- 225-Texto Do Artigo-1533-1457-10-20170915 PDFDocumento7 páginas225-Texto Do Artigo-1533-1457-10-20170915 PDFMarcio SchiavelliAinda não há avaliações
- DR - Thiago Bortolo BianchesiDocumento27 páginasDR - Thiago Bortolo BianchesiBruno GomesAinda não há avaliações
- Modelo POP - Preenchimento Do Formulário de ISSDocumento6 páginasModelo POP - Preenchimento Do Formulário de ISSAnieli SilvaAinda não há avaliações
- Coordenação de Assistência Farmacêutica Na Atenção EspecializadaDocumento6 páginasCoordenação de Assistência Farmacêutica Na Atenção EspecializadaJamile NevesAinda não há avaliações
- Duarte (2010)Documento116 páginasDuarte (2010)Patricia HenriquesAinda não há avaliações
- Cefet-Al 2010 If-Al Professor-Nutricao ProvaDocumento17 páginasCefet-Al 2010 If-Al Professor-Nutricao ProvaCristianeAinda não há avaliações
- Pop AquisiçãoDocumento3 páginasPop AquisiçãoMaria CarolinaAinda não há avaliações
- Pop 08 - Acompanhamento de Temperatura e UmidadeDocumento3 páginasPop 08 - Acompanhamento de Temperatura e UmidadeversadentalfarmaceuticaAinda não há avaliações
- COMUNICADO - Fornecimento Da Vacina Pneumocócica 10-ValenteDocumento2 páginasCOMUNICADO - Fornecimento Da Vacina Pneumocócica 10-ValenteVanderléia LimaAinda não há avaliações
- Nota Tecnica Teste Rapido Covid 13 06 2020Documento12 páginasNota Tecnica Teste Rapido Covid 13 06 2020김형식Ainda não há avaliações
- RQT 851149 Tag 1234Documento47 páginasRQT 851149 Tag 1234Engenharia Clínica HC-UFMGAinda não há avaliações
- Manual Do Fornecedor de Alimentos Sumário PáginasDocumento10 páginasManual Do Fornecedor de Alimentos Sumário PáginasWillian RobertoAinda não há avaliações
- Controlo de Qualidade - Recolha de AmostrasDocumento11 páginasControlo de Qualidade - Recolha de AmostrasLudovina SilvaAinda não há avaliações
- Circular Informativa 07-2020 (DGS-Infarmed) - Vacina BioNTech-Pfizer - ComiRNAtyDocumento3 páginasCircular Informativa 07-2020 (DGS-Infarmed) - Vacina BioNTech-Pfizer - ComiRNAtyenfhelderAinda não há avaliações
- Relatório de Liofilização - FármacosDocumento9 páginasRelatório de Liofilização - FármacosRaniele MirandaAinda não há avaliações
- POP - Manual de ColetaDocumento34 páginasPOP - Manual de ColetaDiógenes L CasimiroAinda não há avaliações
- Timacagro 040720221822265968043Documento2 páginasTimacagro 040720221822265968043Paulo LuanAinda não há avaliações
- Procedimiento Coronavirus PmducDocumento10 páginasProcedimiento Coronavirus PmducFrancisco Encina PerryAinda não há avaliações
- REQ09619 - Formulário para Pedido de Exames de Patologia e TCLE - ÁlvaroDocumento2 páginasREQ09619 - Formulário para Pedido de Exames de Patologia e TCLE - ÁlvarodiagnosesantamariaAinda não há avaliações
- Teste Covid Lepu PDFDocumento5 páginasTeste Covid Lepu PDFclasolanoAinda não há avaliações
- POP 07 Se..Documento4 páginasPOP 07 Se..Karoline FigueiredoAinda não há avaliações
- Implementação Do Plano HACCP Na Gelataria Gelados de PortugalDocumento82 páginasImplementação Do Plano HACCP Na Gelataria Gelados de PortugalelessarodriguesAinda não há avaliações
- Pop Banho No LeitoDocumento4 páginasPop Banho No LeitomichaelbiribaAinda não há avaliações
- Relatório de Estágio 2022Documento14 páginasRelatório de Estágio 2022larissa souzaAinda não há avaliações
- POC3016Documento2 páginasPOC3016Richard AugustoAinda não há avaliações
- Teste Rapido Sifilis, HivDocumento1 páginaTeste Rapido Sifilis, HivJeanEscobarAinda não há avaliações
- Ficha Ilas Sepse 2020Documento1 páginaFicha Ilas Sepse 2020Tiago MaioranoAinda não há avaliações
- Fispq Lava Roupas em Pó EconômicoDocumento6 páginasFispq Lava Roupas em Pó EconômicoMadson PinheiroAinda não há avaliações
- UntitledDocumento5 páginasUntitledJamile NevesAinda não há avaliações
- Guia para Coleta de AmostrasDocumento2 páginasGuia para Coleta de Amostrassantoskaka859Ainda não há avaliações
- Protocolo Coleta e Encaminhamento de Amostras de Swab para Diagnostico de Covid 19Documento4 páginasProtocolo Coleta e Encaminhamento de Amostras de Swab para Diagnostico de Covid 19Leonardo CorreiaAinda não há avaliações
- REQ06710 Temperatura Recebimento de InsumosDocumento1 páginaREQ06710 Temperatura Recebimento de InsumosMatheus RodriguesAinda não há avaliações
- Hemovigilância Do Ato TransfusionalDocumento1 páginaHemovigilância Do Ato TransfusionalAT Canaã dos CarajásAinda não há avaliações
- Pop 33Documento5 páginasPop 33VICTORIA MATTOSAinda não há avaliações
- MicrobiologiaDocumento23 páginasMicrobiologiaAnderson KleberAinda não há avaliações
- Relatório Auditoria NutrifarmDocumento9 páginasRelatório Auditoria NutrifarmNorma FerreiraAinda não há avaliações
- Fispq Lava Louça OiDocumento6 páginasFispq Lava Louça Oinardson100% (1)
- RG: 4425885 SPTC GO: Lote: Validade: Resultado: ÍndiceDocumento7 páginasRG: 4425885 SPTC GO: Lote: Validade: Resultado: Índicedanilfg82Ainda não há avaliações
- Microbiologia Médica II: Esterilização, Diagnóstico Laboratorial e Resposta ImuneNo EverandMicrobiologia Médica II: Esterilização, Diagnóstico Laboratorial e Resposta ImuneNota: 4 de 5 estrelas4/5 (1)
- Templo AyaSofia - Curso Estrela Setenária - Aula 2Documento37 páginasTemplo AyaSofia - Curso Estrela Setenária - Aula 2luamsmarinsAinda não há avaliações
- CursoApometria Auxílio EspiritualDocumento12 páginasCursoApometria Auxílio EspiritualArthur ErpenAinda não há avaliações
- Limpeza Total de EnergiaDocumento11 páginasLimpeza Total de EnergiaGraziele Oliveira BatatinhaAinda não há avaliações
- Gene Keys - Your Life's Work Webinar 14 Nov 2014Documento19 páginasGene Keys - Your Life's Work Webinar 14 Nov 2014luamsmarinsAinda não há avaliações
- 05 GlossarioDocumento77 páginas05 GlossarioluamsmarinsAinda não há avaliações
- ListagemTodososConveniosUnidades-28 03 2022Documento3 páginasListagemTodososConveniosUnidades-28 03 2022mrpezaoAinda não há avaliações
- Aulão AmandaDocumento7 páginasAulão AmandaluamsmarinsAinda não há avaliações
- Ideias de Conteúdo para Se CONECTAR Com Os SEGUIDORESDocumento6 páginasIdeias de Conteúdo para Se CONECTAR Com Os SEGUIDORESThalliny Design100% (1)
- 7 Dragões SagradosDocumento41 páginas7 Dragões SagradosluamsmarinsAinda não há avaliações
- Hexagrama 32: Navegando NA Tormenta: JulgamentoDocumento7 páginasHexagrama 32: Navegando NA Tormenta: JulgamentoluamsmarinsAinda não há avaliações
- Scriptsdevendas Instagramparte 01Documento9 páginasScriptsdevendas Instagramparte 01luamsmarinsAinda não há avaliações
- ESTOICISMODocumento11 páginasESTOICISMOluamsmarinsAinda não há avaliações
- Ideias de Conteudo para Vender Seu ProdutoDocumento3 páginasIdeias de Conteudo para Vender Seu ProdutoluamsmarinsAinda não há avaliações
- Cópia de Scriptsdevendasinstagramparte02Documento8 páginasCópia de Scriptsdevendasinstagramparte02luamsmarinsAinda não há avaliações
- Script Recuperacao Cliente WPPDocumento1 páginaScript Recuperacao Cliente WPPluamsmarinsAinda não há avaliações
- + de 100 Templates Altamente Lucrativos para Seu Feed E Storys E Roteiros de Live E Ainda Templates (Scripts Prontos) para WhatsappDocumento9 páginas+ de 100 Templates Altamente Lucrativos para Seu Feed E Storys E Roteiros de Live E Ainda Templates (Scripts Prontos) para WhatsappluamsmarinsAinda não há avaliações
- Aulão 3 Como Vender Através Dos StoriesDocumento10 páginasAulão 3 Como Vender Através Dos Storiesluamsmarins100% (3)
- E 015 o Que o Yi JingDocumento10 páginasE 015 o Que o Yi JingluamsmarinsAinda não há avaliações
- + 150 Ideias de ConteúdoDocumento17 páginas+ 150 Ideias de ConteúdoPedro Alves100% (1)
- Hexagrama 17: Acompanhando AS Circunstâncias: JulgamentoDocumento6 páginasHexagrama 17: Acompanhando AS Circunstâncias: JulgamentoluamsmarinsAinda não há avaliações
- + de 100 Templates Altamente Lucrativos para Seu Feed E Storys E Roteiros de Live E Ainda Templates (Scripts Prontos) para WhatsappDocumento8 páginas+ de 100 Templates Altamente Lucrativos para Seu Feed E Storys E Roteiros de Live E Ainda Templates (Scripts Prontos) para WhatsappluamsmarinsAinda não há avaliações
- Download-219482-Método Potencialize Insta - Roteiro para Stories BIOINSTAOFICIAL-8136380Documento3 páginasDownload-219482-Método Potencialize Insta - Roteiro para Stories BIOINSTAOFICIAL-8136380luamsmarinsAinda não há avaliações
- Aulão 3 Como Vender Através Dos StoriesDocumento10 páginasAulão 3 Como Vender Através Dos Storiesluamsmarins100% (3)
- Ebook Guia Da Producao de Conteudo para As Redes SociaisDocumento40 páginasEbook Guia Da Producao de Conteudo para As Redes SociaisluamsmarinsAinda não há avaliações
- Ideias de Conteúdo para Se CONECTAR Com Os SEGUIDORESDocumento6 páginasIdeias de Conteúdo para Se CONECTAR Com Os SEGUIDORESThalliny Design100% (1)
- Ideias de Conteudo para Vender Seu ProdutoDocumento3 páginasIdeias de Conteudo para Vender Seu ProdutoluamsmarinsAinda não há avaliações
- 80 - Unimed Vitória - Na05 - Unimed Premium Nacional Coletivo Por Adesao AptDocumento243 páginas80 - Unimed Vitória - Na05 - Unimed Premium Nacional Coletivo Por Adesao AptpessoaanaAinda não há avaliações
- Mapa de QuantidadesDocumento15 páginasMapa de QuantidadesDosmito Joao Desma100% (1)
- Biologia PPT - A Pele HumanaDocumento38 páginasBiologia PPT - A Pele HumanaBiologia ppt100% (1)
- A Dor Da CrucifiCAÇãoDocumento3 páginasA Dor Da CrucifiCAÇãojoselmarezendeAinda não há avaliações
- CARDIOLOGIADocumento17 páginasCARDIOLOGIAMilena CristinaAinda não há avaliações
- Lista de Exerícios 5 - Análise InstrumentalDocumento3 páginasLista de Exerícios 5 - Análise InstrumentalGabriela MoragasAinda não há avaliações
- Anatomia e Fisiologia Da VisãoDocumento4 páginasAnatomia e Fisiologia Da VisãoCláudia Pietrobon100% (1)
- Introdução A Mecanização Agrícola22Documento61 páginasIntrodução A Mecanização Agrícola22Djair Felix0% (1)
- Curso para CIPATRDocumento98 páginasCurso para CIPATRAdony AmorimAinda não há avaliações
- Lista de Exercícios Quimica Geral Eng. Computação AdaptaçãoDocumento4 páginasLista de Exercícios Quimica Geral Eng. Computação AdaptaçãoRenato MartinsAinda não há avaliações
- Aula 01 Veiculos Cosmeticos PDFDocumento32 páginasAula 01 Veiculos Cosmeticos PDFRoberta Medeiros100% (1)
- Ext. Seco Crataegus - Nova LiteraturaDocumento1 páginaExt. Seco Crataegus - Nova LiteraturahowesteveAinda não há avaliações
- FotoproteçãoDocumento12 páginasFotoproteçãoHelen Ferreira linzAinda não há avaliações
- Long JackDocumento2 páginasLong JackAdilmo Sampaio BarbosaAinda não há avaliações
- Sandplay Jogo de AreiaDocumento7 páginasSandplay Jogo de Areianeila mesquita100% (1)
- NeurofibromatoseDocumento24 páginasNeurofibromatoseLucas Gomes de SouzaAinda não há avaliações
- Bqas-Bio Quantum Analysis System 4.8.6.Documento3 páginasBqas-Bio Quantum Analysis System 4.8.6.rexland1Ainda não há avaliações
- Trabalho de Física - Experiência de Eletrização Por ContatoDocumento9 páginasTrabalho de Física - Experiência de Eletrização Por ContatoDaniel CostaAinda não há avaliações
- Ebook Receitas Nanda Castelo BrancoDocumento8 páginasEbook Receitas Nanda Castelo Brancofe.brandaoAinda não há avaliações
- Codex AlimentariusDocumento45 páginasCodex AlimentariusPatrícia EstevesAinda não há avaliações
- Quadriptico FUNCHAL LowDocumento2 páginasQuadriptico FUNCHAL LowAna TeixeiraAinda não há avaliações
- STRALIS 490S40T / 490S44T - 4x2Documento2 páginasSTRALIS 490S40T / 490S44T - 4x2Glauber BrasileiroAinda não há avaliações
- Manejo Reprodutivo de Caprinos e OvinosDocumento139 páginasManejo Reprodutivo de Caprinos e Ovinosderson18Ainda não há avaliações
- Resolve 3Documento24 páginasResolve 3samuel souzaAinda não há avaliações
- Dados Da Fatura de ElectricidadeDocumento3 páginasDados Da Fatura de ElectricidadehermeniodropshippingAinda não há avaliações
- Clinica Ampliada em Saúde MentalDocumento4 páginasClinica Ampliada em Saúde MentalVanessa Caroline DamascenoAinda não há avaliações