Você também pode gostar
- Modelos de LaudosDocumento6 páginasModelos de Laudoswillams AlvesAinda não há avaliações
- Brinquedos PedagogicosDocumento40 páginasBrinquedos PedagogicosCleonice OliveiraAinda não há avaliações
- Processamento de endoscópio: avaliação de dois métodos de limpeza manualNo EverandProcessamento de endoscópio: avaliação de dois métodos de limpeza manualAinda não há avaliações
- NBR 5858 - 1983Documento15 páginasNBR 5858 - 1983telnet837Ainda não há avaliações
- AF121386439414pt BR0701Documento26 páginasAF121386439414pt BR0701camilo obrasAinda não há avaliações
- Cópia de Apresentação1Documento34 páginasCópia de Apresentação1BRUNIHELLY GONZAGAAinda não há avaliações
- Direito Obrigações - Casos Praticos 1Documento16 páginasDireito Obrigações - Casos Praticos 1Esdras J. ReisAinda não há avaliações
- Oncologia Clínica: Curso Preparatório para Prova de Título de Especialista emDocumento376 páginasOncologia Clínica: Curso Preparatório para Prova de Título de Especialista emvitor lopesAinda não há avaliações
- Avaliação - Educação Do Deficiente Físico e Do Múltiplo DeficienteDocumento3 páginasAvaliação - Educação Do Deficiente Físico e Do Múltiplo DeficienteAngelo ParriniAinda não há avaliações
- Gep44 7Documento6 páginasGep44 7Eleandro Jesus GonçalvesAinda não há avaliações
- Glabela en PTDocumento9 páginasGlabela en PTZara Desiree Tonidandel CamposAinda não há avaliações
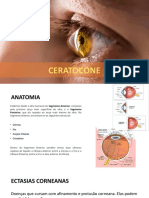
- Queratocone - Diagnóstico e TratamentoDocumento24 páginasQueratocone - Diagnóstico e Tratamentoapi-3742294100% (1)
- Manual de Procedimientos Do Histrico Clinico de Optometria Funcional Da Clinica Universitaria de Sade Visual Final SsDocumento63 páginasManual de Procedimientos Do Histrico Clinico de Optometria Funcional Da Clinica Universitaria de Sade Visual Final SsOPTOGRUPO - OPTOMETRIAAinda não há avaliações
- Ceratocone 1Documento14 páginasCeratocone 1Assane MahamudoAinda não há avaliações
- Bruna TCCDocumento73 páginasBruna TCCCristiane cris hairAinda não há avaliações
- Diretrizes Da CatarataDocumento18 páginasDiretrizes Da CatarataMarcelo FerreiraAinda não há avaliações
- TCC Daniel MonteiroDocumento28 páginasTCC Daniel MonteirojoaoAinda não há avaliações
- TCC Versão FinalDocumento49 páginasTCC Versão FinalBeto Betinho BetoAinda não há avaliações
- Artigo Cristalino para AtvDocumento8 páginasArtigo Cristalino para Atvariannylimadasilva28Ainda não há avaliações
- Cirurgia ParendodonticaDocumento23 páginasCirurgia ParendodonticaOlimpio Barbosa De Oliveira NetoAinda não há avaliações
- Aep - 2 BimDocumento7 páginasAep - 2 BimJessyka SantosAinda não há avaliações
- Mensuração de Tecidos Moles Gengivais Através Do Uso Da Tomografia Computadorizada VolumétricaDocumento68 páginasMensuração de Tecidos Moles Gengivais Através Do Uso Da Tomografia Computadorizada Volumétricagileno pagamentosAinda não há avaliações
- O Transplante de Córneas É Normalmente e Realizado em Pessoas Com Deficiência VisualDocumento2 páginasO Transplante de Córneas É Normalmente e Realizado em Pessoas Com Deficiência VisualTaináAinda não há avaliações
- Monografia AndressaDocumento50 páginasMonografia AndressaHelenitaAinda não há avaliações
- Abordagem Clinico CirurgicaDocumento19 páginasAbordagem Clinico CirurgicaMoisés UrbanoAinda não há avaliações
- 1754-9485 12990Documento10 páginas1754-9485 12990Vitória LeiteAinda não há avaliações
- TFC JonelíDocumento70 páginasTFC Jonelíjonelindjungo5Ainda não há avaliações
- TCC FinalDocumento24 páginasTCC Finalalice.nAinda não há avaliações
- TCC ProntoDocumento59 páginasTCC ProntoBeatriz MouraAinda não há avaliações
- TCC Mariana LonzettiDocumento60 páginasTCC Mariana LonzetticavagnolloisadoraAinda não há avaliações
- TCC 2012 Adriana Trandafilov de AguiarDocumento25 páginasTCC 2012 Adriana Trandafilov de AguiarvaleriaAinda não há avaliações
- Relatório 1 - Estágio (Reparado)Documento7 páginasRelatório 1 - Estágio (Reparado)Soraia AlmeidaAinda não há avaliações
- 174947-Texto Do Artigo Completo-530560-1-10-20211208Documento7 páginas174947-Texto Do Artigo Completo-530560-1-10-20211208Henrique MorettiAinda não há avaliações
- 1998 TCC Acadêmica Tânia Longo Mazzuco - Incidentalomas TireoideanosDocumento54 páginas1998 TCC Acadêmica Tânia Longo Mazzuco - Incidentalomas TireoideanostmazzucoAinda não há avaliações
- Conduta Odontológica Diante Do Paciente em Uso de MedicaçãoDocumento37 páginasConduta Odontológica Diante Do Paciente em Uso de MedicaçãoRubens TeixeiraAinda não há avaliações
- TCC - FinalDocumento34 páginasTCC - FinalLeonardo Tavares de OliveiraAinda não há avaliações
- 33 ReferênciaDocumento101 páginas33 ReferênciaJackAinda não há avaliações
- Tratamento Endodôntico em Sessão ÚnicaDocumento13 páginasTratamento Endodôntico em Sessão ÚnicacceoiapiAinda não há avaliações
- Centro Universitário Regional Do Brasil Odontologia: Salvador 2019Documento50 páginasCentro Universitário Regional Do Brasil Odontologia: Salvador 2019Beatriz MouraAinda não há avaliações
- 2007 CinthiaMendoncadeMeloDocumento116 páginas2007 CinthiaMendoncadeMeloRael Rodrigues Dos SantosAinda não há avaliações
- Projeto - Completo Cam PibicDocumento25 páginasProjeto - Completo Cam PibicAlexandre BragaAinda não há avaliações
- Edema Na Bochecha e MandibulaDocumento45 páginasEdema Na Bochecha e MandibulaEduardo FahidAinda não há avaliações
- Relatorio de Estagio de CirurgiaDocumento8 páginasRelatorio de Estagio de CirurgiaIsabelly RamosAinda não há avaliações
- Protocolo de Regulação de Cirurgias de Catarata Na SES-DFDocumento8 páginasProtocolo de Regulação de Cirurgias de Catarata Na SES-DFRosselyne MouraAinda não há avaliações
- 11 Tipos de Sutura Que Todo Médico Deve Conhecer - PEBMEDDocumento11 páginas11 Tipos de Sutura Que Todo Médico Deve Conhecer - PEBMEDAlfredo MassuanganheAinda não há avaliações
- Cirurgia Radical No Adenocarcinoma GástricoDocumento70 páginasCirurgia Radical No Adenocarcinoma GástricoRenato Accetta100% (2)
- Ricardo HolzchuhDocumento168 páginasRicardo HolzchuhRael Rodrigues Dos SantosAinda não há avaliações
- 5846 24776 1 SMDocumento15 páginas5846 24776 1 SMRebeka SalazarAinda não há avaliações
- PIVICDocumento31 páginasPIVICMaria Vitoria Moreira DantasAinda não há avaliações
- 2010 Dis AaxaguiarDocumento117 páginas2010 Dis AaxaguiarMaira Renata da SilvaAinda não há avaliações
- Artigo Adesivo Fibrina X SuturaDocumento7 páginasArtigo Adesivo Fibrina X SuturaHorst Naconecy de SouzaAinda não há avaliações
- Universidade Federal Do Rio Grande Do Norte Centro de Ciências Da Saúde Departamento de OdontologiaDocumento47 páginasUniversidade Federal Do Rio Grande Do Norte Centro de Ciências Da Saúde Departamento de OdontologiaDa Hae SungAinda não há avaliações
- Ruc,+829 1931 2 PB 1Documento8 páginasRuc,+829 1931 2 PB 1naysellivxAinda não há avaliações
- TCC Revisão NarrativaDocumento26 páginasTCC Revisão NarrativaElisângela CaféAinda não há avaliações
- Andreia Freire MenezesDocumento65 páginasAndreia Freire MenezesRodrigo JesusAinda não há avaliações
- Cópia de Trabalho de Conclusão de Curso WESLAYNEDocumento29 páginasCópia de Trabalho de Conclusão de Curso WESLAYNEWeslayne AlmeidaAinda não há avaliações
- Monografia Roberta Thienne Rosa Da SilvaDocumento28 páginasMonografia Roberta Thienne Rosa Da SilvaGabriel MonteiroAinda não há avaliações
- .Modelo TCC II 2022 Ju e BrenoDocumento24 páginas.Modelo TCC II 2022 Ju e Brenobreno absalonAinda não há avaliações
- Gimenes JuliaHelena TCCDocumento43 páginasGimenes JuliaHelena TCCPablo CardosoAinda não há avaliações
- Relação Dialógica Com o Cliente Sobre Transplante Renal: Cuidado Educativo de EnfermagemDocumento9 páginasRelação Dialógica Com o Cliente Sobre Transplante Renal: Cuidado Educativo de EnfermagemLina SachicaAinda não há avaliações
- Técnicas Radiológicas Fratura de Clavícula em RN's e DosimetriaDocumento21 páginasTécnicas Radiológicas Fratura de Clavícula em RN's e DosimetriaCarlos EduardoAinda não há avaliações
- PERIODONTITEDocumento10 páginasPERIODONTITEluannaapolonioodontoAinda não há avaliações
- Epidemiologia GlaucomaDocumento14 páginasEpidemiologia GlaucomaEduardo SabaAinda não há avaliações
- Radiografia Odontológica DigitalDocumento4 páginasRadiografia Odontológica DigitalMaria MateusAinda não há avaliações
- Schiper SachaPugliese MDocumento67 páginasSchiper SachaPugliese MJuliano BritoAinda não há avaliações
- TCC Eduarda e Suelen VFinal Pós Defesa CertoDocumento27 páginasTCC Eduarda e Suelen VFinal Pós Defesa CertoSabrina da SilvaAinda não há avaliações
- 6 Segundo Molar Inferior Com Anatomia em C - CasoDocumento3 páginas6 Segundo Molar Inferior Com Anatomia em C - CasomarisolatochejaraAinda não há avaliações
- (HÜBNER, 2019) PRODUÇÃO DE CERVEJA ESTILO CATHARINA SOUR COM POLPA DE PITAIA (Hylocereus Polyrhizus) E GENGIBRE (Zingiber Officinale Roscoe)Documento62 páginas(HÜBNER, 2019) PRODUÇÃO DE CERVEJA ESTILO CATHARINA SOUR COM POLPA DE PITAIA (Hylocereus Polyrhizus) E GENGIBRE (Zingiber Officinale Roscoe)vitor auzierAinda não há avaliações
- Origem E Disseminação Dos Microrganismos Do Vinho: Sofia Fernandes CamiloDocumento90 páginasOrigem E Disseminação Dos Microrganismos Do Vinho: Sofia Fernandes CamiloSara CiriacoAinda não há avaliações
- (Bezerra, 2016) EFEITO DE DIFERENTES PROCESSOS DE SANITIZAÇÃO DE FRUTOS DE AÇAÍ Na Qualidade Microbiologica e Fisico QuimicaDocumento200 páginas(Bezerra, 2016) EFEITO DE DIFERENTES PROCESSOS DE SANITIZAÇÃO DE FRUTOS DE AÇAÍ Na Qualidade Microbiologica e Fisico Quimicavitor auzierAinda não há avaliações
- (CAMPOS, 2017) Compostos Bioativos em Produtos Lácteos Adicionados de Polpa de Açaí e Camu-Camu Suplementados Com Bactérias ProbióticasDocumento117 páginas(CAMPOS, 2017) Compostos Bioativos em Produtos Lácteos Adicionados de Polpa de Açaí e Camu-Camu Suplementados Com Bactérias Probióticasvitor auzierAinda não há avaliações
- (CARDOSO, 2021) Desenvolvimento de Duas Formulações Base de Cerveja Estilo Sour Keffir e KombuchaDocumento13 páginas(CARDOSO, 2021) Desenvolvimento de Duas Formulações Base de Cerveja Estilo Sour Keffir e Kombuchavitor auzierAinda não há avaliações
- (Da Silva, 2021) Cerveja Especial - Catharina Sour e Fruit BeerDocumento39 páginas(Da Silva, 2021) Cerveja Especial - Catharina Sour e Fruit Beervitor auzierAinda não há avaliações
- (Irwin, 2001) 67243.en - PTDocumento9 páginas(Irwin, 2001) 67243.en - PTvitor auzierAinda não há avaliações
- (Trujillo, 2010) 33150-Texto Del Artículo-122901-1-10-20120913.es - PTDocumento11 páginas(Trujillo, 2010) 33150-Texto Del Artículo-122901-1-10-20120913.es - PTvitor auzierAinda não há avaliações
- (CUBA, 2011) ESTILO DE VIDA ALIMENTAÇÃO ATIV FISICA E SOBREPESO EM MEDICOS - Es.ptDocumento6 páginas(CUBA, 2011) ESTILO DE VIDA ALIMENTAÇÃO ATIV FISICA E SOBREPESO EM MEDICOS - Es.ptvitor auzierAinda não há avaliações
- (Peeters, 2014) Health Care Costs Associated With Prolonged Sitting and Inactivity - En.ptDocumento25 páginas(Peeters, 2014) Health Care Costs Associated With Prolonged Sitting and Inactivity - En.ptvitor auzierAinda não há avaliações
- (Suija, 2010) 1471-2296-11-48.en - PTDocumento6 páginas(Suija, 2010) 1471-2296-11-48.en - PTvitor auzierAinda não há avaliações
- Ementa Analise Sensorial e Off FlavorsDocumento1 páginaEmenta Analise Sensorial e Off Flavorsvitor auzierAinda não há avaliações
- Meloxicam em CãesDocumento3 páginasMeloxicam em Cãesvitor auzierAinda não há avaliações
- Relatório de EstagioDocumento14 páginasRelatório de EstagioCastro Naldo0% (1)
- Fichas: Texto PublicitárioDocumento3 páginasFichas: Texto Publicitárioanon_1271374050% (1)
- Alcoolismo No TrabalhoDocumento18 páginasAlcoolismo No TrabalhoJuliana SouzaAinda não há avaliações
- giroscópio2012editadoPDF (Roteiro) III PDFDocumento8 páginasgiroscópio2012editadoPDF (Roteiro) III PDFxotunredmailtopAinda não há avaliações
- Ebook Estratégias Que Eu Usei para Faturar Mais de 10k Por MêsDocumento61 páginasEbook Estratégias Que Eu Usei para Faturar Mais de 10k Por Mêsju.balanAinda não há avaliações
- 5 Documentários Brasileiros para Se Refletir Sobre EducaçãoDocumento5 páginas5 Documentários Brasileiros para Se Refletir Sobre EducaçãoAparecida De Fatima Gomes MacaubasAinda não há avaliações
- Curriculo de Ensino BasicoDocumento103 páginasCurriculo de Ensino BasicoDelio Patricio Tura DanielAinda não há avaliações
- Exercicios - 2 - AlgoritmosDocumento3 páginasExercicios - 2 - AlgoritmosPedro CândidoAinda não há avaliações
- Despesas CaiãoDocumento6 páginasDespesas CaiãoCaio VitalAinda não há avaliações
- Modelo de Petição de Ação de Indenização Por Danos MateriaisDocumento5 páginasModelo de Petição de Ação de Indenização Por Danos Materiaisgraciele AlkmimAinda não há avaliações
- Manual Aspirador Electronia BST-803 Calipso - 3117828Documento16 páginasManual Aspirador Electronia BST-803 Calipso - 3117828Selenita VoshinAinda não há avaliações
- Formação Serviço AlentejoDocumento125 páginasFormação Serviço AlentejoCrisAinda não há avaliações
- BIKEFIT v6.0Documento1 páginaBIKEFIT v6.0airtonpaulo2Ainda não há avaliações
- 12.07 - PortuguesDocumento9 páginas12.07 - PortuguesMarcos HenriqueAinda não há avaliações
- Egito AntigoDocumento3 páginasEgito AntigoMarcio Martins de SouzaAinda não há avaliações
- Apostila Irrigação 2012Documento77 páginasApostila Irrigação 2012anon_140267718Ainda não há avaliações
- Plano de Ensino PDFDocumento3 páginasPlano de Ensino PDFIdna AlencarAinda não há avaliações
- Marvel RPGDocumento6 páginasMarvel RPGChaulin Diogo da CostaAinda não há avaliações
- 2.7 Aula de Laboratório de Anatomia Do Olho e Do Ouvido 2020 Dra. Leny Van SwaaijDocumento6 páginas2.7 Aula de Laboratório de Anatomia Do Olho e Do Ouvido 2020 Dra. Leny Van SwaaijNorvaldo PedroAinda não há avaliações
- A Importância Da SeletividadeDocumento5 páginasA Importância Da SeletividadeSergio Ricardo NobreAinda não há avaliações
- Apostila Fazendo Seu Dicionario de AcordesDocumento8 páginasApostila Fazendo Seu Dicionario de AcordesNelson PedonAinda não há avaliações
- Quest Biolcel Prova 1Documento6 páginasQuest Biolcel Prova 1oidualc20110% (1)
- Manual UFCD3539-alteradoDocumento31 páginasManual UFCD3539-alteradoClara RamalhoAinda não há avaliações