Você também pode gostar
- Boletim Tecnico 100 PDFDocumento88 páginasBoletim Tecnico 100 PDFmiguelmenegazzo80% (5)
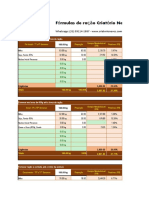
- (Criatorio Neves) - Fórmula RacaoDocumento31 páginas(Criatorio Neves) - Fórmula RacaoMatheus100% (1)
- Fosforo em Solo e Planta em Condições TropicaisDocumento123 páginasFosforo em Solo e Planta em Condições Tropicaispenelope13130% (1)
- Imunologia Da Cárie Dentária !!!Documento12 páginasImunologia Da Cárie Dentária !!!AMANDA MARIA SOUZA DE ALBUQUERQUEAinda não há avaliações
- Fluor Na Odontopediatria 2012tenutachedidcurymitosevidenciasodontopDocumento45 páginasFluor Na Odontopediatria 2012tenutachedidcurymitosevidenciasodontopJoão Henrique100% (1)
- Unidade27 FT EtiologiaDocumento8 páginasUnidade27 FT EtiologiaMarina SouzaAinda não há avaliações
- Apostila de CaldoDocumento46 páginasApostila de CaldoPatriqui Estela100% (3)
- Nutricao ParenteralDocumento51 páginasNutricao ParenteralFaculdade de Farmácia da UFF100% (3)
- Fundamentos para Assistncia Odontolgica IDocumento5 páginasFundamentos para Assistncia Odontolgica IMarcelo HaggeAinda não há avaliações
- Periodontia em OdontopediatriaDocumento6 páginasPeriodontia em OdontopediatriaGiovanna VitóriaAinda não há avaliações
- O Que É Hipovitaminose ADocumento5 páginasO Que É Hipovitaminose ALoyanne TelesAinda não há avaliações
- Periodontia NP1Documento4 páginasPeriodontia NP1Josiane GamaAinda não há avaliações
- Atividade - Manifestações Orais de Doenças SistêmicasDocumento2 páginasAtividade - Manifestações Orais de Doenças SistêmicasLaura CaetanoAinda não há avaliações
- A MostraDocumento6 páginasA MostraJardel SantosAinda não há avaliações
- Anomalias Do DesenvolvimentoDocumento5 páginasAnomalias Do DesenvolvimentoMatheus MacollyAinda não há avaliações
- Etiologia Das MaloclusõesDocumento4 páginasEtiologia Das MaloclusõeswalfaiaAinda não há avaliações
- Efeitos Metabólicos DasDocumento13 páginasEfeitos Metabólicos DasSilvelita MeteloAinda não há avaliações
- Amostra PDFDocumento6 páginasAmostra PDFJonas SousaAinda não há avaliações
- Periodontia ResumoDocumento19 páginasPeriodontia ResumoJoão AlvesAinda não há avaliações
- Periodontia ResumoDocumento19 páginasPeriodontia ResumoJoão Alves100% (1)
- 1 PBDocumento5 páginas1 PBmarina6pereira6h6ppiAinda não há avaliações
- Agravos em Saúde BucalDocumento82 páginasAgravos em Saúde BucalFelipe Nicolau50% (2)
- ISEC - Fissura Lábio PalatinaDocumento5 páginasISEC - Fissura Lábio PalatinaJuliaBeatriz7Ainda não há avaliações
- Avitaminose ADocumento23 páginasAvitaminose ASadjy IssaAinda não há avaliações
- Livro FlúorDocumento26 páginasLivro FlúorWillams AlfaiaAinda não há avaliações
- Exercícios de Revisão 1 Avaliação REC SAÚDE BUCAL SBB3Documento76 páginasExercícios de Revisão 1 Avaliação REC SAÚDE BUCAL SBB3Marcello MazzaroAinda não há avaliações
- Recuperação VitaminasDocumento2 páginasRecuperação VitaminaspatriciaAinda não há avaliações
- 8 Periodontia I e Periodontia II - 165 183 PDFDocumento19 páginas8 Periodontia I e Periodontia II - 165 183 PDFKelma BrandaoAinda não há avaliações
- Bônus Questões Vitaminas e MineraisDocumento31 páginasBônus Questões Vitaminas e MineraisLenise PrankeAinda não há avaliações
- Classificação Das DPDocumento4 páginasClassificação Das DPIsla RodriguesAinda não há avaliações
- Principais Agravos em Saúde BucalDocumento29 páginasPrincipais Agravos em Saúde BucalShayana Paes MartinsAinda não há avaliações
- Bioquímica Na OdontologiaDocumento41 páginasBioquímica Na OdontologiaAna Carolina MachadoAinda não há avaliações
- Apresentação 1Documento18 páginasApresentação 1Breno ZorzoAinda não há avaliações
- Periodontia 1Documento5 páginasPeriodontia 1Maria AparecidaAinda não há avaliações
- Aula 1Documento106 páginasAula 1csbentaquiAinda não há avaliações
- Aula 1 - Introdução À CariologiaDocumento38 páginasAula 1 - Introdução À CariologiaAlissa KinAinda não há avaliações
- Carências NutricionaisDocumento32 páginasCarências NutricionaisMaikol Tiago Ribeiro100% (2)
- Disturbios GastricosDocumento33 páginasDisturbios GastricosAna Virginia SousaAinda não há avaliações
- 8 Periodontia I e Periodontia II - 165 183Documento19 páginas8 Periodontia I e Periodontia II - 165 183vitoria lorrayneAinda não há avaliações
- Complexo 05 Amelia EtiologiaDocumento9 páginasComplexo 05 Amelia EtiologiaVívianChagasSilvaAinda não há avaliações
- 8 Periodontia I e Periodontia II 165 183Documento19 páginas8 Periodontia I e Periodontia II 165 183Leticia Rodrigues CorreiaAinda não há avaliações
- ATIVIDADES DE EDUCAÇÃO EM SAÚDE PARA AlunosDocumento42 páginasATIVIDADES DE EDUCAÇÃO EM SAÚDE PARA AlunosDaniele Castro AguiarAinda não há avaliações
- Acc Etiologia Da CárieDocumento3 páginasAcc Etiologia Da CárieNaiara RibeiroAinda não há avaliações
- Aula 8 - Doenças PeriodontaisDocumento16 páginasAula 8 - Doenças PeriodontaissarahcamillyalvesAinda não há avaliações
- Resumo 3Documento4 páginasResumo 3Denis Félix GuedesAinda não há avaliações
- AmelogenesDocumento6 páginasAmelogenesJosiane GamaAinda não há avaliações
- Cabeça e PescoçoDocumento5 páginasCabeça e PescoçoEmilly GomesAinda não há avaliações
- Micronutrientes Vitaminas e MineraisDocumento12 páginasMicronutrientes Vitaminas e MineraisTainara MendonçaAinda não há avaliações
- Und 1 Seç 1Documento21 páginasUnd 1 Seç 1Jonnathan Oliveira ReisAinda não há avaliações
- Unidade27 FT Etiologia PDFDocumento8 páginasUnidade27 FT Etiologia PDFMateus MatosAinda não há avaliações
- Vitamina ADocumento7 páginasVitamina ACatiane Cabral100% (1)
- Slide 1.1 - Anomalias Congênitas, Síndromes e Manifestações OraisDocumento20 páginasSlide 1.1 - Anomalias Congênitas, Síndromes e Manifestações OraisCristiano BatisteliAinda não há avaliações
- Síndrome de Pierre RobinDocumento2 páginasSíndrome de Pierre RobinPaula LarissaAinda não há avaliações
- Fatores Predisponentes e Modificadores Das Doenças Biofilme Dependentes (Recuperação Automática)Documento6 páginasFatores Predisponentes e Modificadores Das Doenças Biofilme Dependentes (Recuperação Automática)brunaletcarmangAinda não há avaliações
- Trabalho Sobre CárieDocumento20 páginasTrabalho Sobre Cárienilvia_danieleAinda não há avaliações
- Atividades de Educação em Saúde para Os AlunosDocumento43 páginasAtividades de Educação em Saúde para Os AlunosDaniele Castro AguiarAinda não há avaliações
- Bioquimica Da CarieDocumento8 páginasBioquimica Da CarieIvan Vieira da SilvaAinda não há avaliações
- Terapia Nutricional Crianças Com Fissura LabiopalativaDocumento18 páginasTerapia Nutricional Crianças Com Fissura LabiopalativaLuna SousaAinda não há avaliações
- Cárie Dentária e Doenças PeriodontaisDocumento12 páginasCárie Dentária e Doenças PeriodontaisAna LúciaAinda não há avaliações
- Fissura Labial 1Documento18 páginasFissura Labial 1João Luiz Vilela GarciaAinda não há avaliações
- Roteiro de Aula Classificação Das Doenças PeriodontaisDocumento2 páginasRoteiro de Aula Classificação Das Doenças PeriodontaisFrancisco PintoAinda não há avaliações
- Etiologia Das Maloclusões TUDODocumento8 páginasEtiologia Das Maloclusões TUDODanilo MandariniAinda não há avaliações
- Microbiologia OralDocumento7 páginasMicrobiologia OralAllana BarrosoAinda não há avaliações
- Reações teciduais frente à movimentação dentária ortodóntica e suas implicações clínicasNo EverandReações teciduais frente à movimentação dentária ortodóntica e suas implicações clínicasEditora PUC MinasAinda não há avaliações
- Tumores BenignosDocumento150 páginasTumores BenignoslilianaAinda não há avaliações
- 2 - Malformações Orais e Maxilofaciais 2Documento71 páginas2 - Malformações Orais e Maxilofaciais 2lilianaAinda não há avaliações
- Patologia Potencialmente MalignaDocumento126 páginasPatologia Potencialmente MalignalilianaAinda não há avaliações
- Aula TP 18 - 03Documento56 páginasAula TP 18 - 03lilianaAinda não há avaliações
- Aula TP 29 - 04Documento61 páginasAula TP 29 - 04lilianaAinda não há avaliações
- Aula ODP TP 13 - 05Documento40 páginasAula ODP TP 13 - 05lilianaAinda não há avaliações
- Moodle - TP - Controlo de Placa - 2 - 11 - PPTXDocumento16 páginasMoodle - TP - Controlo de Placa - 2 - 11 - PPTXlilianaAinda não há avaliações
- Produção de Ácido FosfóricoDocumento156 páginasProdução de Ácido FosfóricoDaiany BarbosaAinda não há avaliações
- Seja Doutor Da Sua Soja PotafosDocumento6 páginasSeja Doutor Da Sua Soja PotafosLafaieteLopesAinda não há avaliações
- Alterações Do Equilíbrio Ácido-Base - Formação de InternosDocumento75 páginasAlterações Do Equilíbrio Ácido-Base - Formação de InternosPedro Rodriguez Diaz100% (1)
- Relatorio de Estagio - Ana Rita Da Costa Rocha PDFDocumento78 páginasRelatorio de Estagio - Ana Rita Da Costa Rocha PDFCoach LeonardAinda não há avaliações
- Trabalho de QuimicaDocumento9 páginasTrabalho de Quimicakm seriesAinda não há avaliações
- Apostila de Jardinagem - Projeto "Semeando Oportunidades"Documento102 páginasApostila de Jardinagem - Projeto "Semeando Oportunidades"andre bailone100% (5)
- 02 - Colocando A Mão Na MassaDocumento32 páginas02 - Colocando A Mão Na MassajeanAinda não há avaliações
- Detoxificando Os Rins JornadaDocumento61 páginasDetoxificando Os Rins Jornadaalessandro01viniciusAinda não há avaliações
- Alimentação Vacas LeiteirasDocumento62 páginasAlimentação Vacas LeiteirasJosé CostaAinda não há avaliações
- Manejo Da Cana de AçucarDocumento16 páginasManejo Da Cana de AçucarGrasieli RodriguesAinda não há avaliações
- Resumo PATOLOGIASDocumento56 páginasResumo PATOLOGIASBruna MoreiraAinda não há avaliações
- Suplemento CaninoDocumento14 páginasSuplemento CaninoGustavo LealAinda não há avaliações
- Aula de Claudicação EquinaDocumento4 páginasAula de Claudicação EquinaJuliana LorettiAinda não há avaliações
- Como Montar Sua DietaDocumento31 páginasComo Montar Sua DietaCotebizza LuizAinda não há avaliações
- Vinagre de Maçã VivoDocumento13 páginasVinagre de Maçã Vivoeevargas50Ainda não há avaliações
- Dosagens de Cálcio e Fósforo Séricos e UrinárioDocumento4 páginasDosagens de Cálcio e Fósforo Séricos e UrinárioBio.Unip.Marques100% (1)
- Formulacao de Misturas Minerais para BovinosDocumento18 páginasFormulacao de Misturas Minerais para BovinosMozar MedeirosAinda não há avaliações
- Água e Sais Minerais Com ExercíciosDocumento7 páginasÁgua e Sais Minerais Com ExercíciosandreiaserpaAinda não há avaliações
- Como Cuidar de Eguas PrenhesDocumento4 páginasComo Cuidar de Eguas PrenhesGabriellevetAinda não há avaliações
- Guedes Oliveira e Carvalho 2018 Efeitos Deletérios Do Tempo Prolongado No Leito Nos Sistemas CorporaisDocumento8 páginasGuedes Oliveira e Carvalho 2018 Efeitos Deletérios Do Tempo Prolongado No Leito Nos Sistemas CorporaisLaís MedeirosAinda não há avaliações
- Sistemas Agroflorestais e Desenvolvimento PDFDocumento348 páginasSistemas Agroflorestais e Desenvolvimento PDFsatgrouppAinda não há avaliações
- Ciclo Do FosforoDocumento11 páginasCiclo Do FosforoAna Paula ZuzaAinda não há avaliações
- Nutrição BovinaDocumento89 páginasNutrição BovinaSamir Bandeira100% (1)
- Ciclo Do FósforoDocumento6 páginasCiclo Do Fósforohillbill2009100% (2)
- Artigo Cientifico - UniVitoriaDocumento10 páginasArtigo Cientifico - UniVitoriaDouglas BatistaAinda não há avaliações